Diefenbach Russell J, Lee Jenny H, Stewart Ashleigh, Menzies Alexander M, Carlino Matteo S, Saw Robyn P M, Stretch Jonathan R, Long Georgina V, Scolyer Richard A, Rizos Helen
Macquarie Medical School, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, NSW, Australia.
Melanoma Institute Australia, The University of Sydney, Sydney, NSW, Australia.
Front Oncol. 2022 Apr 12;12:820510. doi: 10.3389/fonc.2022.820510. eCollection 2022.
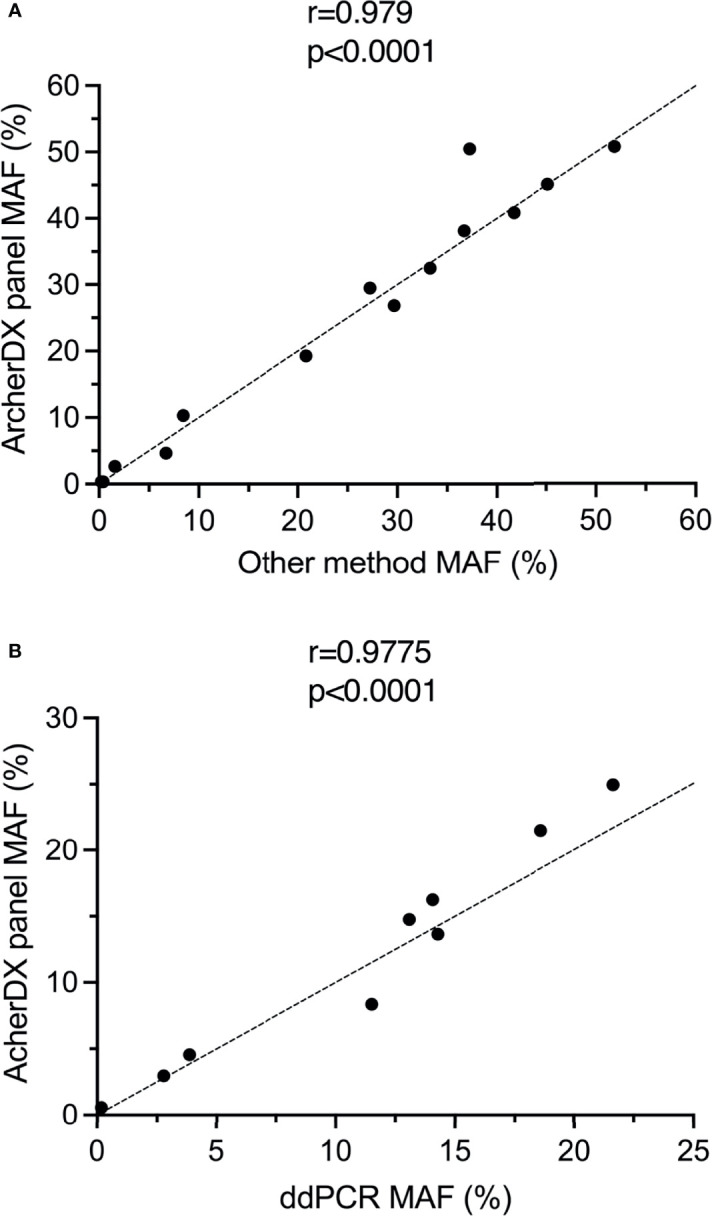
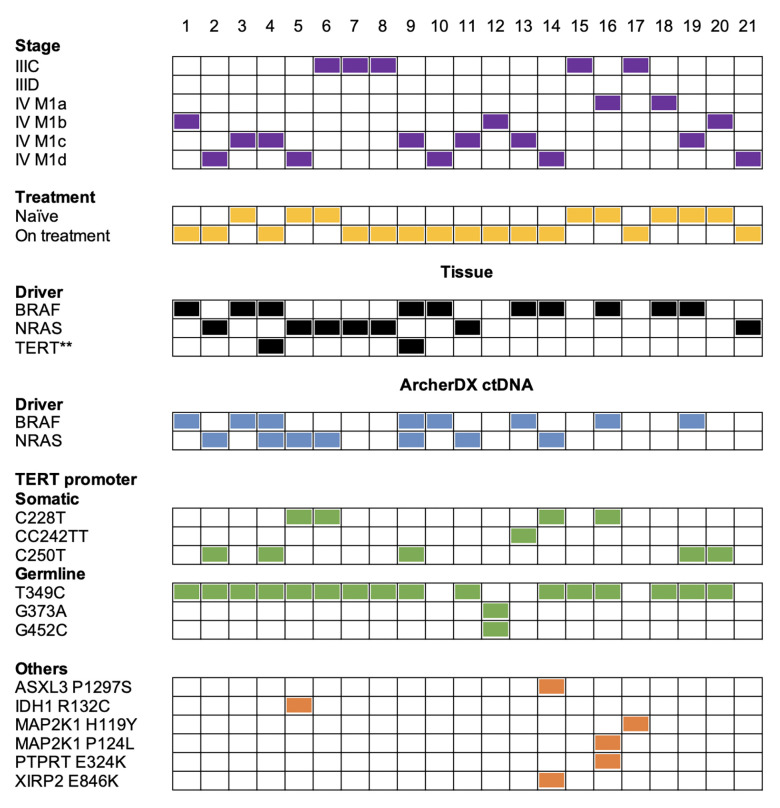
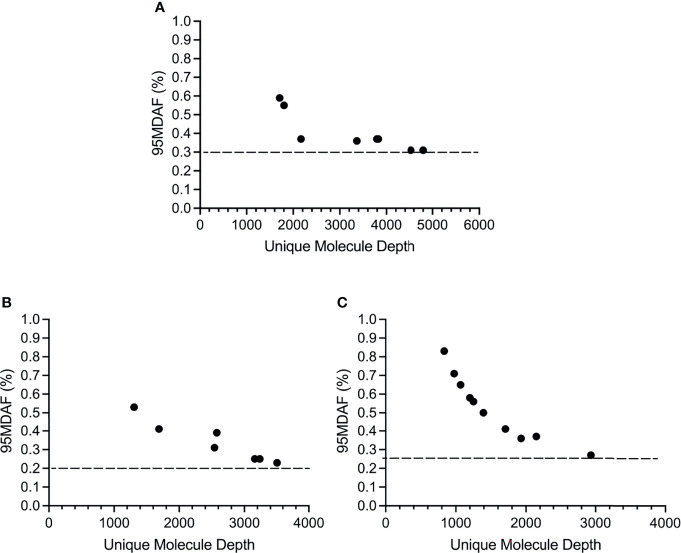
Detection of melanoma mutations using circulating tumor DNA (ctDNA) is a potential alternative to using genomic DNA from invasive tissue biopsies. To date, mutations in the GC-rich promoter region, which is commonly mutated in melanoma, have been technically difficult to detect in ctDNA using next-generation sequencing (NGS) panels. In this study, we developed a custom melanoma NGS panel for detection of ctDNA, which encompasses the top 15 gene mutations in melanoma including the promoter. We analyzed 21 stage III and IV melanoma patient samples who were treatment-naïve or on therapy. The overall detection rate of the custom panel, based on // promoter mutations, was 14/21 (67%) patient samples which included a C250T mutation in one and mutation negative sample. A or mutation was detected in the ctDNA of 13/21 (62%) patients while promoter mutations were detected in 10/21 (48%) patients. Co-occurrence of promoter mutations with or mutations was found in 9/10 (90%) patients. The custom ctDNA panel showed a concordance of 16/21 (76%) with tissue based-detection and included 12 / mutation positive and 4 mutation negative patients. The ctDNA mutation detection rate for stage IV was 12/16 (75%) and for stage III was 1/5 (20%). Based on , and promoter mutations, the custom melanoma panel displayed a limit of detection of ~0.2% mutant allele frequency and showed significant correlation with droplet digital PCR. For one patient, a novel MAP2K1 H119Y mutation was detected in an promoter mutation negative background. To increase the detection rate to >90% for stage IV melanoma patients, we plan to expand our custom panel to 50 genes. This study represents one of the first to successfully detect promoter mutations in ctDNA from cutaneous melanoma patients using a targeted NGS panel.
利用循环肿瘤DNA(ctDNA)检测黑色素瘤突变是一种有潜力的替代方法,可替代使用侵入性组织活检获取的基因组DNA。迄今为止,富含GC的启动子区域(黑色素瘤中常见突变区域)中的突变,使用下一代测序(NGS)面板在ctDNA中进行检测在技术上存在困难。在本研究中,我们开发了一种用于检测ctDNA的定制黑色素瘤NGS面板,该面板涵盖了黑色素瘤中前15个基因突变,包括启动子。我们分析了21例III期和IV期黑色素瘤患者样本,这些患者未接受过治疗或正在接受治疗。基于启动子突变,定制面板的总体检测率为14/21(67%)患者样本,其中包括1例患者的C250T突变和1例突变阴性样本。13/21(62%)患者的ctDNA中检测到A或B突变,而10/21(48%)患者检测到启动子突变。在9/10(90%)患者中发现启动子突变与A或B突变同时存在。定制ctDNA面板与基于组织的检测一致性为16/21(76%),包括12例A/B突变阳性和4例A/B突变阴性患者。IV期的ctDNA突变检测率为12/16(75%),III期为1/5(20%)。基于A、B和启动子突变,定制黑色素瘤面板显示检测限约为0.2%突变等位基因频率,并且与液滴数字PCR显示出显著相关性。对于1例患者,在启动子突变阴性背景下检测到一种新的MAP2K1 H119Y突变。为了将IV期黑色素瘤患者的检测率提高到>90%,我们计划将定制面板扩展到50个基因。本研究是首批使用靶向NGS面板成功检测皮肤黑色素瘤患者ctDNA中启动子突变的研究之一。