Department of Pulmonary and Critical Care Medicine, Qingdao Municipal Hospital Group, Qingdao City, Shandong Province, 266011, People's Republic of China.
Department of Infectious Diseases, Nanjing Lishui People's Hospital, Nanjing City, Jiangsu Province, 211213, People's Republic of China.
Clin Interv Aging. 2022 Apr 23;17:603-614. doi: 10.2147/CIA.S356925. eCollection 2022.
Limited data were available about the burden of cardiovascular events (CVEs) during hospitalization in elderly patients with community-acquired pneumonia (CAP). The aim was to assess the incidence, characteristics, predictive factors and outcomes of CVEs in elderly patients with CAP during hospitalization.
This study was a multicenter, retrospective research on hospitalized elderly patients with CAP from the CAP-China network. Predictive factors for the occurrence of CVEs and 30-day mortality were identified by multivariable logistic regression analysis.
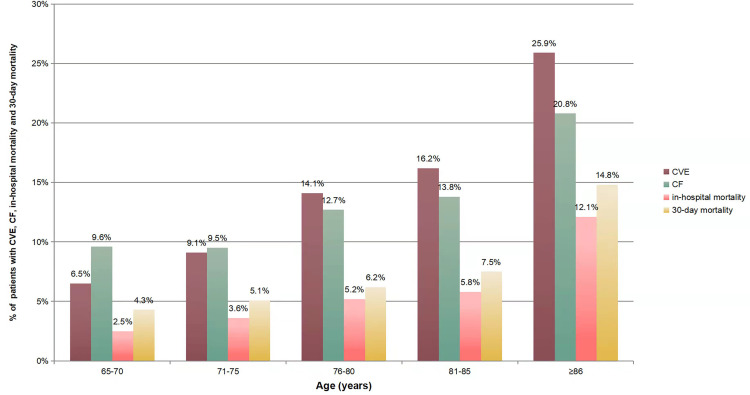
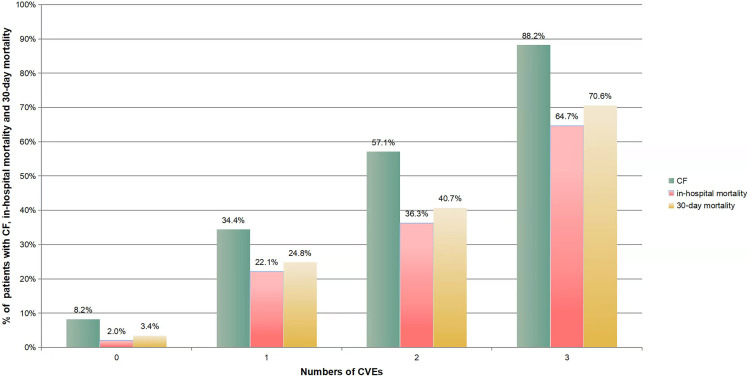
Of 2941 hospitalized elderly patients, 402 (13.7%) developed CVEs during hospitalization with the median age of 81 years old. Compared with non-CVEs patients, patients with CVEs were older, more comorbidities, and higher disease severity; use of glucocorticoids, leukocytosis, azotemia, hyponatremia, multilobe infiltration and pleural effusion were more common; the rate of clinical failure (CF), in-hospital mortality and 30-day mortality were higher, which significantly increased with age and the number of CVEs (p < 0.001). Multivariable logistic regression showed previous history of congestive heart failure (odds ratio [OR], 6.16; 95% CI, 4.14-9.18), CF (OR, 4.69; 95% CI, 3.392-6.48), previous history of ischemic heart disease (OR, 2.22; 95% CI, 1.61-3.07), use of glucocorticoids (OR, 2.0; 95% CI, 1.39-2.89), aspiration (OR, 1.88; 95% CI, 1.26-2.81), pleural effusion (OR, 1.66; 95% CI, 1.25-2.20), multilobe infiltration (OR, 1.50; 95% CI, 1.15-1.96), age (OR, 1.05; 95% CI, 1.04-1.07), and blood urea nitrogen (OR, 1.03; 95% CI, 1.01-1.06) were independent predictors for the occurrence of CVEs, while level of blood sodium (OR, 0.98; 95% CI, 0.97-0.99) was protective factor. Renal failure (OR, 9.46; 95% CI, 4.17-21.48), respiratory failure (OR, 9.32; 95% CI, 5.91-14.71), sepsis/septic shock (OR, 7.87; 95% CI, 3.58-17.31), new cerebrovascular diseases (OR, 5.94; 95% CI, 1.78-19.87), new heart failure (OR, 4.04; 95% CI, 1.15-14.14), new arrhythmia (OR, 2.38; 95% CI, 1.11-5.14), aspiration (OR, 1.95; 95% CI, 1.09-3.50), CURB-65 (OR, 1.57; 95% CI, 1.21-2.02), and white blood cell count (OR, 1.05; 95% CI, 1.02-1.09) were independent predictors for 30-day mortality in elderly patients with CAP, while lymphocyte count (OR, 0.63; 95% CI, 0.46-0.87) was protective factor.
Patients with CVEs had heavier disease burden and worse prognosis. Early recognition of risk factors is meaningful to strengthen the management in elderly patients with CAP.
关于老年社区获得性肺炎(CAP)患者住院期间心血管事件(CVE)的负担,数据有限。本研究旨在评估老年 CAP 患者住院期间 CVE 的发生率、特征、预测因素和结局。
本研究是一项多中心、回顾性研究,纳入了来自 CAP-China 网络的老年 CAP 住院患者。使用多变量逻辑回归分析确定发生 CVE 和 30 天死亡率的预测因素。
在 2941 名住院老年患者中,402 名(13.7%)发生了住院期间 CVE,中位年龄为 81 岁。与非 CVE 患者相比,CVE 患者年龄更大,合并症更多,疾病严重程度更高;更常使用糖皮质激素、白细胞增多、氮质血症、低钠血症、多叶浸润和胸腔积液;临床失败(CF)、住院死亡率和 30 天死亡率更高,且随着年龄和 CVE 数量的增加而显著增加(p<0.001)。多变量逻辑回归显示,充血性心力衰竭(OR,6.16;95%CI,4.14-9.18)、CF(OR,4.69;95%CI,3.392-6.48)、缺血性心脏病(OR,2.22;95%CI,1.61-3.07)、使用糖皮质激素(OR,2.0;95%CI,1.39-2.89)、吸入(OR,1.88;95%CI,1.26-2.81)、胸腔积液(OR,1.66;95%CI,1.25-2.20)、多叶浸润(OR,1.50;95%CI,1.15-1.96)、年龄(OR,1.05;95%CI,1.04-1.07)和血尿素氮(OR,1.03;95%CI,1.01-1.06)是发生 CVE 的独立预测因素,而血钠水平(OR,0.98;95%CI,0.97-0.99)是保护因素。肾衰竭(OR,9.46;95%CI,4.17-21.48)、呼吸衰竭(OR,9.32;95%CI,5.91-14.71)、脓毒症/感染性休克(OR,7.87;95%CI,3.58-17.31)、新发脑血管疾病(OR,5.94;95%CI,1.78-19.87)、新发心力衰竭(OR,4.04;95%CI,1.15-14.14)、新发心律失常(OR,2.38;95%CI,1.11-5.14)、吸入(OR,1.95;95%CI,1.09-3.50)、CURB-65(OR,1.57;95%CI,1.21-2.02)和白细胞计数(OR,1.05;95%CI,1.02-1.09)是老年 CAP 患者 30 天死亡率的独立预测因素,而淋巴细胞计数(OR,0.63;95%CI,0.46-0.87)是保护因素。
发生 CVE 的患者疾病负担更重,预后更差。早期识别危险因素对加强老年 CAP 患者的管理具有重要意义。