Sia Ching-Hui, Ko Junsuk, Zheng Huili, Ho Andrew Fu-Wah, Foo David, Foo Ling-Li, Lim Patrick Zhan-Yun, Liew Boon Wah, Chai Ping, Yeo Tiong-Cheng, Yip James W L, Chua Terrance, Chan Mark Yan-Yee, Tan Jack Wei Chieh, Figtree Gemma, Bulluck Heerajnarain, Hausenloy Derek J
Department of Cardiology, National University Heart Centre Singapore, Singapore, Singapore.
Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Front Cardiovasc Med. 2022 Apr 14;9:876465. doi: 10.3389/fcvm.2022.876465. eCollection 2022.
Acute myocardial infarction (AMI) cases have decreased in part due to the advent of targeted therapies for standard modifiable cardiovascular disease risk factors (SMuRF). Recent studies have reported that ST-elevation myocardial infarction (STEMI) patients without SMuRF (termed "SMuRF-less") may be increasing in prevalence and have worse outcomes than "SMuRF-positive" patients. As these studies have been limited to STEMI and comprised mainly Caucasian cohorts, we investigated the changes in the prevalence and mortality of both SMuRF-less STEMI and non-STEMI (NSTEMI) patients in a multiethnic Asian population.
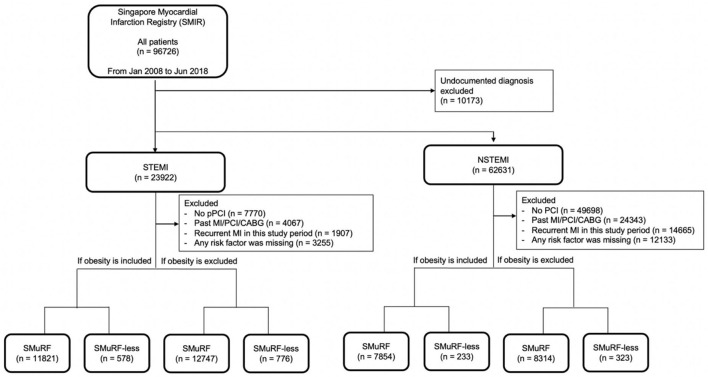
We evaluated 23,922 STEMI and 62,631 NSTEMI patients from a national multiethnic registry. Short-term cardiovascular and all-cause mortalities in SMuRF-less patients were compared to SMuRF-positive patients.
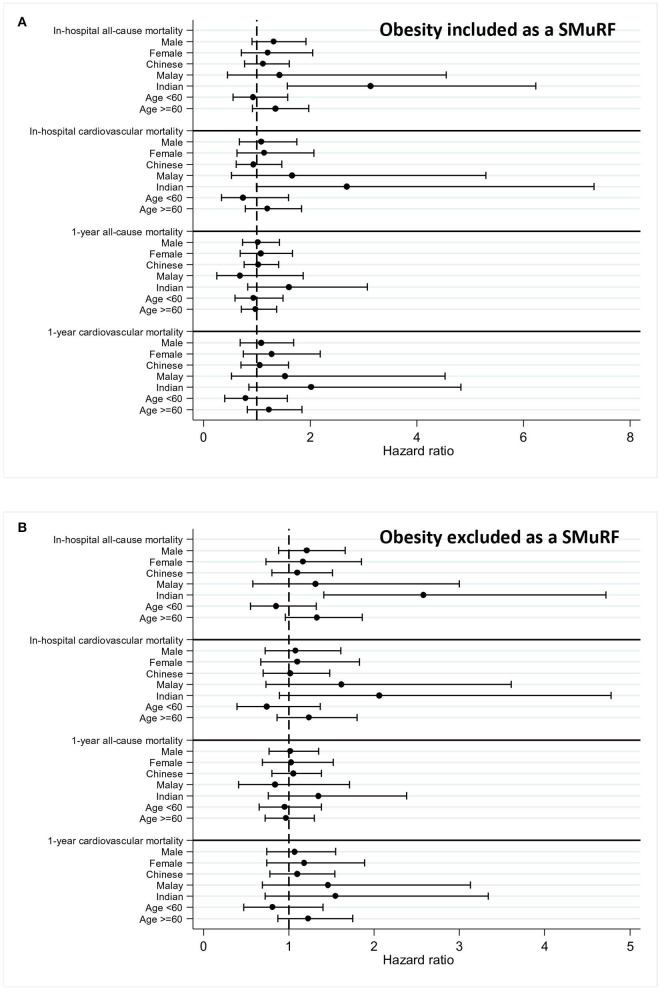
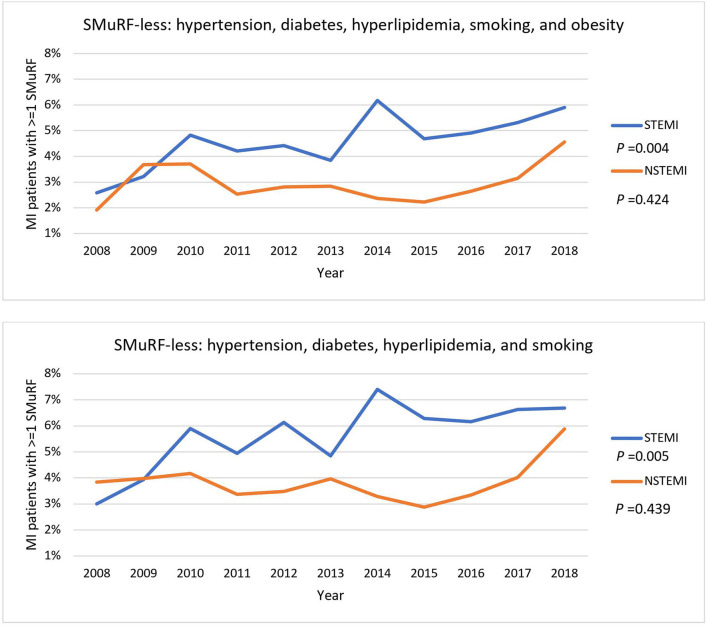
The proportions of SMuRF-less STEMI but not of NSTEMI have increased over the years. In hospitals, all-cause and cardiovascular mortality and 1-year cardiovascular mortality were significantly higher in SMuRF-less STEMI after adjustment for age, creatinine, and hemoglobin. However, this difference did not remain after adjusting for anterior infarction, cardiopulmonary resuscitation (CPR), and Killip class. There were no differences in mortality in SMuRF-less NSTEMI. In contrast to Chinese and Malay patients, SMuRF-less patients of South Asian descent had a two-fold higher risk of in-hospital all-cause mortality even after adjusting for features of increased disease severity.
SMuRF-less patients had an increased risk of mortality with STEMI, suggesting that there may be unidentified nonstandard risk factors predisposing SMuRF-less patients to a worse prognosis. This group of patients may benefit from more intensive secondary prevention strategies to improve clinical outcomes.
急性心肌梗死(AMI)病例有所减少,部分原因是针对标准可改变心血管疾病风险因素(SMuRF)的靶向治疗的出现。最近的研究报告称,没有SMuRF的ST段抬高型心肌梗死(STEMI)患者(称为“无SMuRF”)的患病率可能在增加,并且比“有SMuRF”的患者预后更差。由于这些研究仅限于STEMI且主要包括白种人队列,我们调查了多民族亚洲人群中无SMuRF的STEMI和非STEMI(NSTEMI)患者的患病率和死亡率变化。
我们评估了来自全国多民族登记处的23922例STEMI患者和62631例NSTEMI患者。将无SMuRF患者的短期心血管和全因死亡率与有SMuRF的患者进行比较。
多年来,无SMuRF的STEMI患者比例有所增加,但无SMuRF的NSTEMI患者比例未增加。在医院中,调整年龄、肌酐和血红蛋白后,无SMuRF的STEMI患者的全因死亡率、心血管死亡率和1年心血管死亡率显著更高。然而,在调整前壁梗死、心肺复苏(CPR)和Killip分级后,这种差异不再存在。无SMuRF的NSTEMI患者的死亡率没有差异。与华裔和马来裔患者不同,即使在调整疾病严重程度增加的特征后,南亚裔无SMuRF的患者院内全因死亡风险仍高出两倍。
无SMuRF的STEMI患者死亡风险增加,这表明可能存在未被识别的非标准风险因素,使无SMuRF的患者预后更差。这组患者可能受益于更强化的二级预防策略以改善临床结局。