Department of Cardiology, Lithuanian University of Health Sciences Hospital Kauno Klinikos, Lithuania.
Lithuanian University of Health Sciences, Lithuania.
Perfusion. 2023 Sep;38(6):1288-1297. doi: 10.1177/02676591221100739. Epub 2022 May 3.
To find the imaging mortality predictors in patients with previous myocardial infarction (MI), symptomatic heart failure (HF), and reduced left ventricle (LV) ejection fraction (EF).
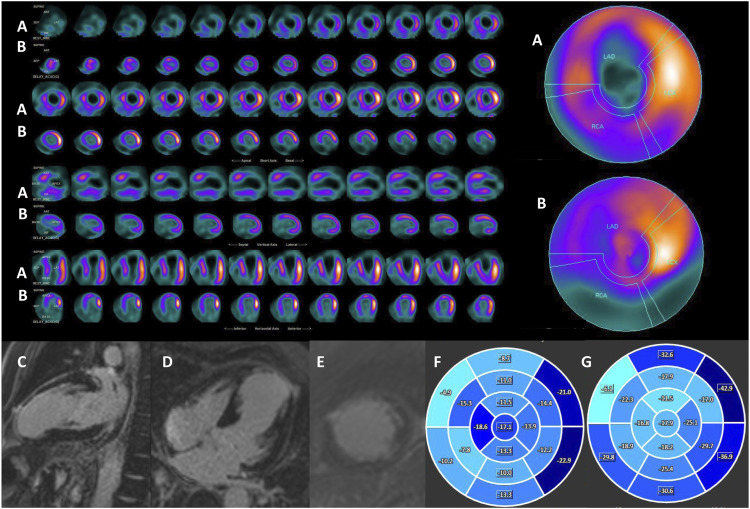
for the study 39 patients were selected prospectively with prior MI, symptomatic HF, and LVEF ≤40%. All patients underwent transthoracic echocardiography (TTE), single-photon emission computed tomography myocardial perfusion imaging (SPECT MPI), 18F-FDG positron emission tomography (FDG PET). 31 patients underwent cardiovascular magnetic resonance (CMR) with late gadolinium enhancement (LGE). Patients were divided into two groups: 1 group - cardiac death; 2 group - no cardiac death. Myocardial scars were assessed on a 5-point-scale. Follow-up data was obtained.
Imaging features disclosed significant difference ( < 0.05) of defect score (CMR and SPECT-PET), LV end-diastolic diameter (EDD) (TTE), LVEDD index (CMR), LV global longitudinal strain (CMR) and LV global circumferential strain (CMR) between the groups. Predictors of cardiac death were: LVEDD index (TTE) and LV global longitudinal strain. The cut-off values to predict cardiac death were: defect score (CMR) 25 (AUC, 79.5%; OR 1.8, 95% CI 1.2-2.7), SPECT-PET defect score 22 (AUC, 73.9%; OR 0.5, 95% CI 0.3-0.7), LVEDD (TTE) 58 mm (AUC, 88.4%; OR 23.6, 95% CI 2.6-217.7), LVEDDi 30 mm/m (TTE) (AUC, 73.6%; OR 22.0, 95% CI 1.9-251.5), LVEDDi 33.6 mm/m (CMR) (AUC, 73.6%; OR 22.0, 95% CI 1.9-251.5), LV global longitudinal strain -13.4 (AUC, 87.8%; OR 2.1, 95% CI 1.2-3.7) and LV global circumferential strain -16.3 (AUC, 76.1%; OR 1.9, 95% CI 1.2-3.0).
Imaging features, such as defect score (CMR) >25, SPECT-PET defect score >22, LVEDD (TTE) >58 mm, LVEDDi (TTE) >30 mm/m, LVEDDi (CMR) >33.6 mm/m, LV global longitudinal strain -13.4 and LV global circumferential strain -16.3, may increase sensitivity and specificity of FDG PET and LGE CMR predicting of late mortality.
寻找有既往心肌梗死(MI)、有症状心力衰竭(HF)和左心室射血分数(LVEF)降低的患者的影像学死亡预测因子。
前瞻性选择了 39 例有既往 MI、有症状 HF 和 LVEF≤40%的患者。所有患者均接受了经胸超声心动图(TTE)、单光子发射计算机断层扫描心肌灌注成像(SPECT MPI)、18F-FDG 正电子发射断层扫描(FDG PET)。31 例患者接受了心脏磁共振(CMR)检查,并进行了钆延迟增强(LGE)。患者被分为两组:1 组——心脏死亡;2 组——无心脏死亡。评估心肌瘢痕的 5 分制评分。获取随访数据。
两组之间的缺陷评分(CMR 和 SPECT-PET)、LV 舒张末期直径(EDD)(TTE)、LVEDD 指数(CMR)、LV 整体纵向应变(CMR)和 LV 整体周向应变(CMR)存在显著差异(<0.05)。心脏死亡的预测因子为:LVEDD 指数(TTE)和 LV 整体纵向应变。预测心脏死亡的截断值为:CMR 的缺陷评分 25(AUC,79.5%;OR 1.8,95%CI 1.2-2.7)、SPECT-PET 的缺陷评分 22(AUC,73.9%;OR 0.5,95%CI 0.3-0.7)、TTE 的 LVEDD 58mm(AUC,88.4%;OR 23.6,95%CI 2.6-217.7)、TTE 的 LVEDDi 30mm/m(AUC,73.6%;OR 22.0,95%CI 1.9-251.5)、CMR 的 LVEDDi 33.6mm/m(AUC,73.6%;OR 22.0,95%CI 1.9-251.5)、LV 整体纵向应变-13.4(AUC,87.8%;OR 2.1,95%CI 1.2-3.7)和 LV 整体周向应变-16.3(AUC,76.1%;OR 1.9,95%CI 1.2-3.0)。
CMR 上的缺陷评分>25、SPECT-PET 上的缺陷评分>22、TTE 上的 LVEDD>58mm、TTE 上的 LVEDDi>30mm/m、CMR 上的 LVEDDi>33.6mm/m、LV 整体纵向应变-13.4 和 LV 整体周向应变-16.3 等影像学特征可能会提高 FDG PET 和 LGE CMR 预测晚期死亡率的敏感性和特异性。