Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, California, USA; Monash Cardiovascular Research Centre, Victorian Heart Institute, Monash University and MonashHeart, Monash Health, Melbourne, Victoria, Australia.
Cardiovascular Imaging Research Center, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
JACC Cardiovasc Imaging. 2022 May;15(5):859-871. doi: 10.1016/j.jcmg.2021.11.016. Epub 2022 Jan 12.
The aim of this study was to precisely phenotype culprit and nonculprit lesions in myocardial infarction (MI) and lesions in stable coronary artery disease (CAD) using coronary computed tomography angiography (CTA)-based radiomic analysis.
It remains debated whether any single coronary atherosclerotic plaque within the vulnerable patient exhibits unique morphology conferring an increased risk of clinical events.
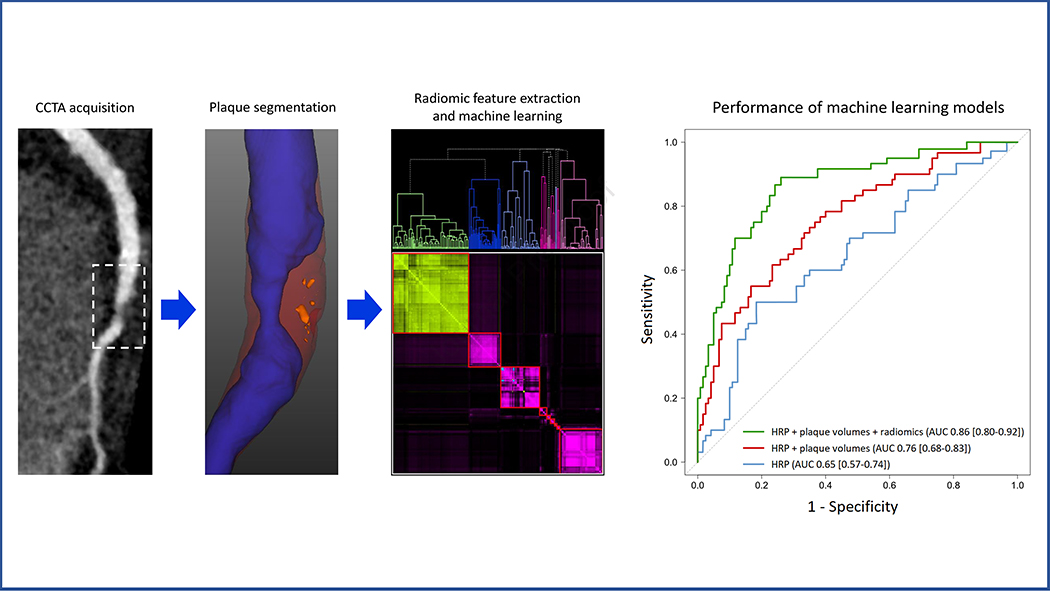
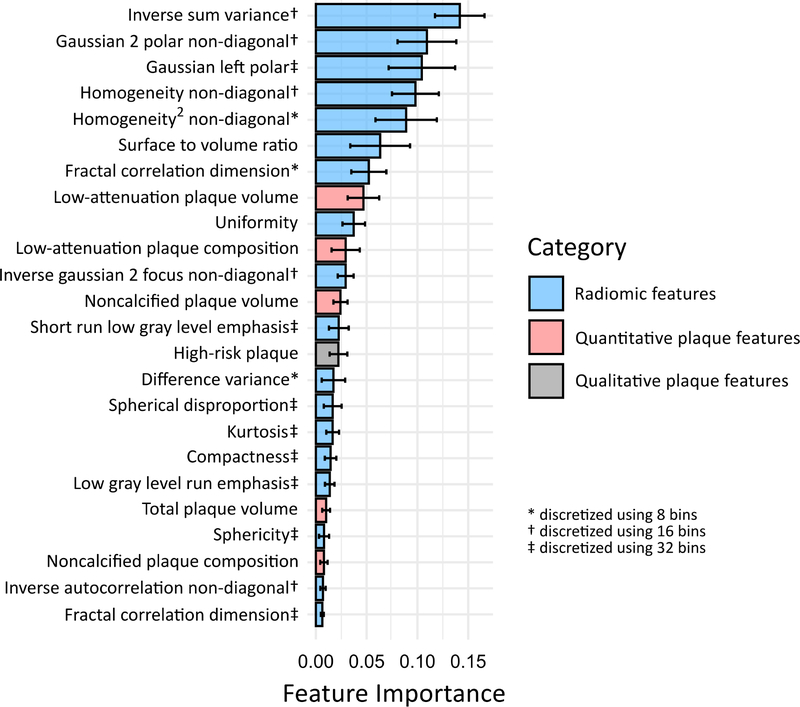
A total of 60 patients with acute MI prospectively underwent coronary CTA before invasive angiography and were matched to 60 patients with stable CAD. For all coronary lesions, high-risk plaque (HRP) characteristics were qualitatively assessed, followed by semiautomated plaque quantification and extraction of 1,103 radiomic features. Machine learning models were built to examine the additive value of radiomic features for discriminating culprit lesions over and above HRP and plaque volumes.
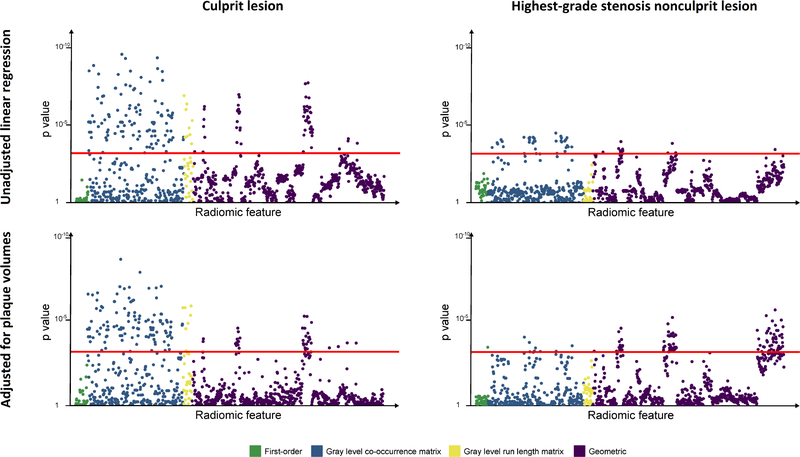
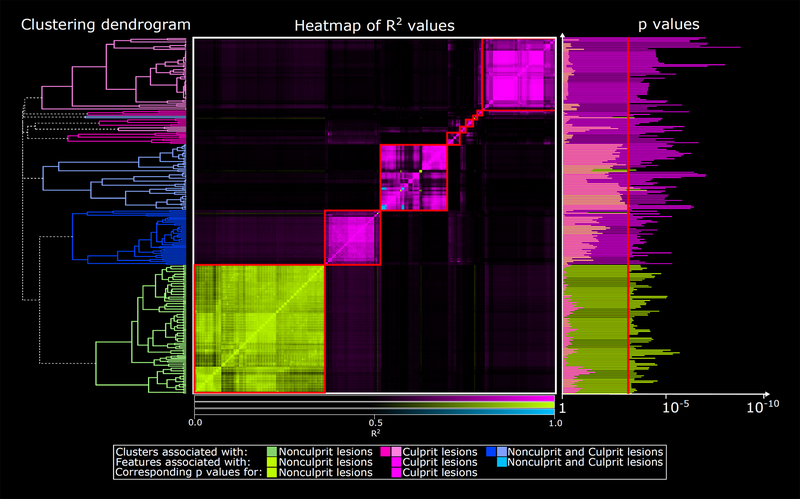
Culprit lesions had higher mean volumes of noncalcified plaque (NCP) and low-density noncalcified plaque (LDNCP) compared with the highest-grade stenosis nonculprits and highest-grade stenosis stable CAD lesions (NCP: 138.1 mm vs 110.7 mm vs 102.7 mm; LDNCP: 14.2 mm vs 9.8 mm vs 8.4 mm; both P < 0.01). In multivariable linear regression adjusted for NCP and LDNCP volumes, 14.9% (164 of 1,103) of radiomic features were associated with culprits and 9.7% (107 of 1,103) were associated with the highest-grade stenosis nonculprits (critical P < 0.0007) when compared with highest-grade stenosis stable CAD lesions as reference. Hierarchical clustering of significant radiomic features identified 9 unique data clusters (latent phenotypes): 5 contained radiomic features specific to culprits, 1 contained features specific to highest-grade stenosis nonculprits, and 3 contained features associated with either lesion type. Radiomic features provided incremental value for discriminating culprit lesions when added to a machine learning model containing HRP and plaque volumes (area under the receiver-operating characteristic curve 0.86 vs 0.76; P = 0.004).
Culprit lesions and highest-grade stenosis nonculprit lesions in MI have distinct radiomic signatures compared with lesions in stable CAD. Within the vulnerable patient may exist individual vulnerable plaques identifiable by coronary CTA-based precision phenotyping.
本研究旨在通过基于冠状动脉计算机断层扫描血管造影(CTA)的放射组学分析,精确表型心肌梗死(MI)中的罪犯和非罪犯病变以及稳定型冠状动脉疾病(CAD)中的病变。
目前仍存在争议,即易损患者体内的任何单个冠状动脉粥样硬化斑块是否具有独特的形态,从而增加临床事件的风险。
前瞻性纳入 60 例急性 MI 患者,在进行有创血管造影前进行冠状动脉 CTA 检查,并与 60 例稳定型 CAD 患者相匹配。对所有冠状动脉病变进行高风险斑块(HRP)特征的定性评估,然后进行半自动斑块定量和提取 1103 个放射组学特征。构建机器学习模型,以检查放射组学特征在区分罪犯病变方面的附加价值,超过 HRP 和斑块体积。
与最高狭窄度非罪犯病变和最高狭窄度稳定 CAD 病变相比,罪犯病变的非钙化斑块(NCP)和低密度非钙化斑块(LDNCP)平均体积更高(NCP:138.1mm 比 110.7mm 比 102.7mm;LDNCP:14.2mm 比 9.8mm 比 8.4mm;均 P<0.01)。在多变量线性回归中,校正 NCP 和 LDNCP 体积后,14.9%(1103 个中的 164 个)的放射组学特征与罪犯病变相关,9.7%(1103 个中的 107 个)与最高狭窄度非罪犯病变相关(临界 P<0.0007),以最高狭窄度稳定 CAD 病变作为参考。对显著放射组学特征进行层次聚类,可识别出 9 个独特的数据簇(潜在表型):5 个簇包含与罪犯病变特异性相关的放射组学特征,1 个簇包含与最高狭窄度非罪犯病变特异性相关的特征,3 个簇包含与两种病变类型均相关的特征。当放射组学特征添加到包含 HRP 和斑块体积的机器学习模型中时,可为区分罪犯病变提供附加价值(接受者操作特征曲线下面积 0.86 比 0.76;P=0.004)。
MI 中的罪犯病变和最高狭窄度非罪犯病变与稳定 CAD 中的病变具有明显不同的放射组学特征。在易损患者中,可能存在可通过基于冠状动脉 CTA 的精准表型识别的个体易损斑块。