Hussein Mohamed, González-Bueno Puyal Juana, Lines David, Sehgal Vinay, Toth Daniel, Ahmad Omer F, Kader Rawen, Everson Martin, Lipman Gideon, Fernandez-Sordo Jacobo Ortiz, Ragunath Krish, Esteban Jose Miguel, Bisschops Raf, Banks Matthew, Haefner Michael, Mountney Peter, Stoyanov Danail, Lovat Laurence B, Haidry Rehan
Division of Surgery and Interventional Sciences, University College London, London, UK.
Wellcome/EPSRC Centre for Interventional and Surgical Sciences (WEISS), University College London, London, UK.
United European Gastroenterol J. 2022 Jul;10(6):528-537. doi: 10.1002/ueg2.12233. Epub 2022 May 6.
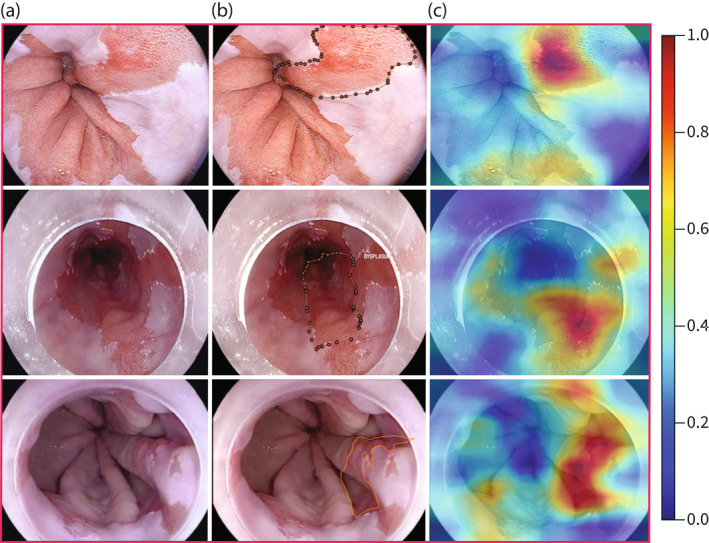
Seattle protocol biopsies for Barrett's Esophagus (BE) surveillance are labour intensive with low compliance. Dysplasia detection rates vary, leading to missed lesions. This can potentially be offset with computer aided detection. We have developed convolutional neural networks (CNNs) to identify areas of dysplasia and where to target biopsy.
119 Videos were collected in high-definition white light and optical chromoendoscopy with i-scan (Pentax Hoya, Japan) imaging in patients with dysplastic and non-dysplastic BE (NDBE). We trained an indirectly supervised CNN to classify images as dysplastic/non-dysplastic using whole video annotations to minimise selection bias and maximise accuracy. The CNN was trained using 148,936 video frames (31 dysplastic patients, 31 NDBE, two normal esophagus), validated on 25,161 images from 11 patient videos and tested on 264 iscan-1 images from 28 dysplastic and 16 NDBE patients which included expert delineations. To localise targeted biopsies/delineations, a second directly supervised CNN was generated based on expert delineations of 94 dysplastic images from 30 patients. This was tested on 86 i-scan one images from 28 dysplastic patients.
The indirectly supervised CNN achieved a per image sensitivity in the test set of 91%, specificity 79%, area under receiver operator curve of 93% to detect dysplasia. Per-lesion sensitivity was 100%. Mean assessment speed was 48 frames per second (fps). 97% of targeted biopsy predictions matched expert and histological assessment at 56 fps. The artificial intelligence system performed better than six endoscopists.
Our CNNs classify and localise dysplastic Barrett's Esophagus potentially supporting endoscopists during surveillance.
用于巴雷特食管(BE)监测的西雅图方案活检劳动强度大且依从性低。发育异常的检出率各不相同,导致病变漏诊。计算机辅助检测有可能弥补这一问题。我们开发了卷积神经网络(CNN)来识别发育异常区域以及活检靶点。
收集了119段高清白光和采用i-scan(日本宾得霍亚公司)成像的光学染色内镜检查视频,这些视频来自发育异常和非发育异常BE(NDBE)患者。我们训练了一个间接监督的CNN,利用整个视频注释将图像分类为发育异常/非发育异常,以尽量减少选择偏倚并最大化准确性。该CNN使用148,936个视频帧(31名发育异常患者、31名NDBE患者、两名正常食管患者)进行训练,在来自11名患者视频的25,161张图像上进行验证,并在来自28名发育异常患者和16名NDBE患者的264张i-scan-1图像上进行测试,其中包括专家划定区域。为了定位靶向活检/划定区域,基于30名患者的94张发育异常图像的专家划定区域,生成了第二个直接监督的CNN。这在来自28名发育异常患者的86张i-scan one图像上进行了测试。
间接监督的CNN在测试集中检测发育异常时,每张图像的灵敏度为91%,特异性为79%,受试者操作特征曲线下面积为93%。每个病变的灵敏度为100%。平均评估速度为每秒48帧(fps)。97%的靶向活检预测在56 fps时与专家和组织学评估结果相符。人工智能系统的表现优于六名内镜医师。
我们的CNN对发育异常的巴雷特食管进行分类和定位,可能在监测过程中为内镜医师提供支持。