Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy.
Department of Anesthesia and Intensive Care Units, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy.
Crit Care. 2022 May 7;26(1):127. doi: 10.1186/s13054-022-03996-0.
Prone positioning improves survival in moderate-to-severe acute respiratory distress syndrome (ARDS) unrelated to the novel coronavirus disease (COVID-19). This benefit is probably mediated by a decrease in alveolar collapse and hyperinflation and a more homogeneous distribution of lung aeration, with fewer harms from mechanical ventilation. In this preliminary physiological study we aimed to verify whether prone positioning causes analogue changes in lung aeration in COVID-19. A positive result would support prone positioning even in this other population.
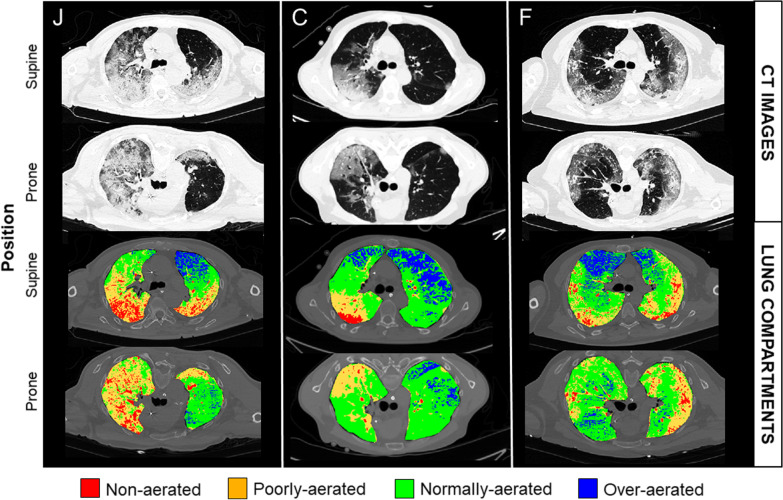
Fifteen mechanically-ventilated patients with COVID-19 underwent a lung computed tomography in the supine and prone position with a constant positive end-expiratory pressure (PEEP) within three days of endotracheal intubation. Using quantitative analysis, we measured the volume of the non-aerated, poorly-aerated, well-aerated, and over-aerated compartments and the gas-to-tissue ratio of the ten vertical levels of the lung. In addition, we expressed the heterogeneity of lung aeration with the standardized median absolute deviation of the ten vertical gas-to-tissue ratios, with lower values indicating less heterogeneity.
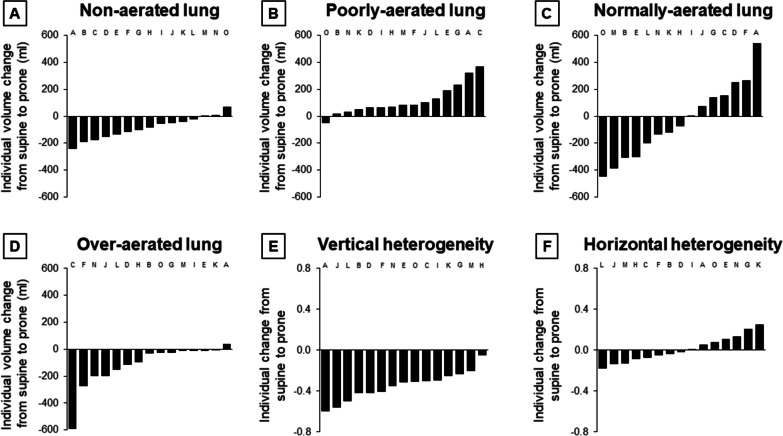
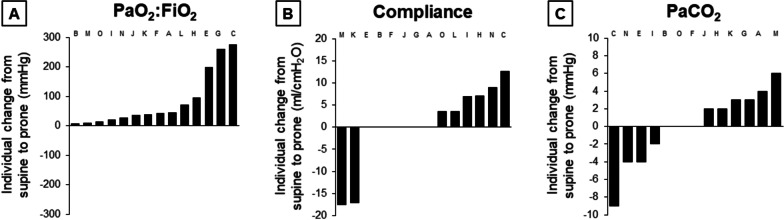
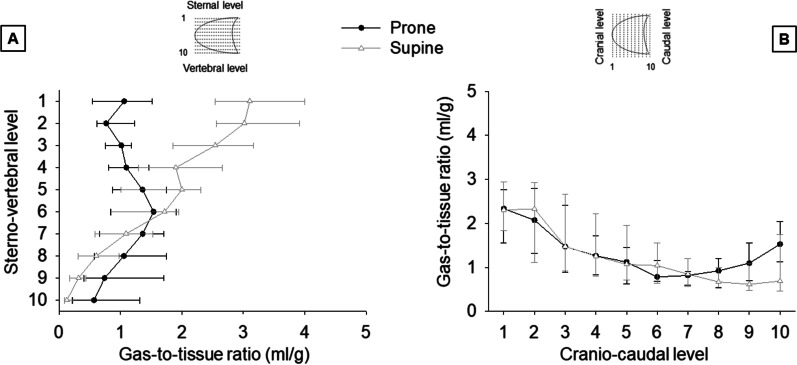
By the time of the study, PEEP was 12 (10-14) cmHO and the PaO:FiO 107 (84-173) mmHg in the supine position. With prone positioning, the volume of the non-aerated compartment decreased by 82 (26-147) ml, of the poorly-aerated compartment increased by 82 (53-174) ml, of the normally-aerated compartment did not significantly change, and of the over-aerated compartment decreased by 28 (11-186) ml. In eight (53%) patients, the volume of the over-aerated compartment decreased more than the volume of the non-aerated compartment. The gas-to-tissue ratio of the ten vertical levels of the lung decreased by 0.34 (0.25-0.49) ml/g per level in the supine position and by 0.03 (- 0.11 to 0.14) ml/g in the prone position (p < 0.001). The standardized median absolute deviation of the gas-to-tissue ratios of those ten levels decreased in all patients, from 0.55 (0.50-0.71) to 0.20 (0.14-0.27) (p < 0.001).
In fifteen patients with COVID-19, prone positioning decreased alveolar collapse, hyperinflation, and homogenized lung aeration. A similar response has been observed in other ARDS, where prone positioning improves outcome. Therefore, our data provide a pathophysiological rationale to support prone positioning even in COVID-19.
俯卧位可改善与新型冠状病毒病(COVID-19)无关的中重度急性呼吸窘迫综合征(ARDS)患者的生存率。这种益处可能是通过减少肺泡萎陷和过度充气以及更均匀地分布肺通气来实现的,同时机械通气的危害也更小。在这项初步的生理学研究中,我们旨在验证俯卧位是否会导致 COVID-19 患者的肺通气发生类似的变化。阳性结果将支持即使在这种其他人群中也采用俯卧位。
15 名接受机械通气的 COVID-19 患者在气管插管后 3 天内以恒定的呼气末正压(PEEP)进行仰卧位和俯卧位肺部计算机断层扫描。使用定量分析,我们测量了未充气、充气不良、充气良好和过度充气的区域的体积以及肺的十个垂直层面的气体与组织比。此外,我们用十个垂直层面气体与组织比的标准化中值绝对偏差来表示肺通气的异质性,较小的值表示异质性较低。
在研究时,仰卧位的 PEEP 为 12(10-14)cmH2O,PaO:FiO 为 107(84-173)mmHg。采用俯卧位时,未充气区域的体积减少了 82(26-147)ml,充气不良区域的体积增加了 82(53-174)ml,充气良好区域的体积没有明显变化,过度充气区域的体积减少了 28(11-186)ml。在 8 名(53%)患者中,过度充气区域的体积减少量超过了未充气区域的体积。肺的十个垂直层面的气体与组织比在仰卧位时每层面降低 0.34(0.25-0.49)ml/g,在俯卧位时降低 0.03(-0.11 至 0.14)ml/g(p<0.001)。所有患者的十个层面的气体与组织比的标准化中值绝对偏差均降低,从 0.55(0.50-0.71)降至 0.20(0.14-0.27)(p<0.001)。
在 15 名 COVID-19 患者中,俯卧位减少了肺泡萎陷、过度充气和肺通气均匀化。在其他 ARDS 中也观察到类似的反应,俯卧位改善了预后。因此,我们的数据为支持俯卧位提供了病理生理学依据,即使是在 COVID-19 中也是如此。