Unit for Anaesthesiological Investigations, Division of Anaesthesiology, Department of Anaesthesiology, Pharmacology, Intensive Care and Emergency Medicine, University Hospitals of Geneva and University of Geneva, Rue Willy Donzé 6, 1205, Geneva, Switzerland.
Department of Internal Medicine, University Hospitals of Geneva, Geneva, Switzerland.
Sci Rep. 2022 Jun 30;12(1):11085. doi: 10.1038/s41598-022-15122-9.
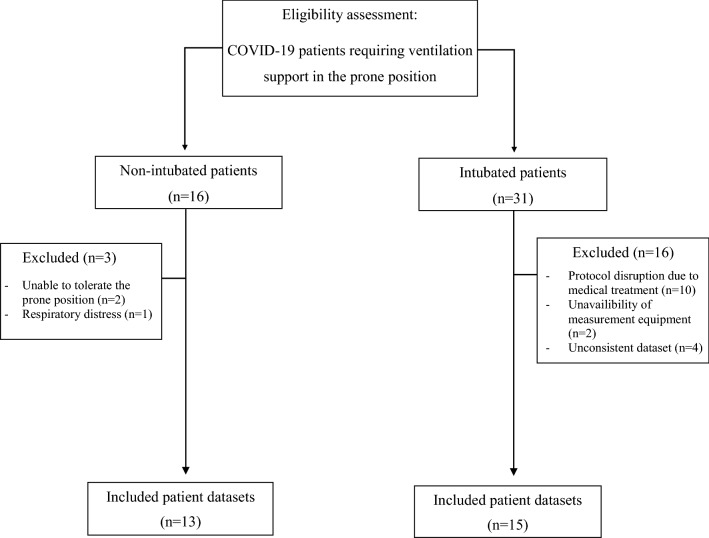
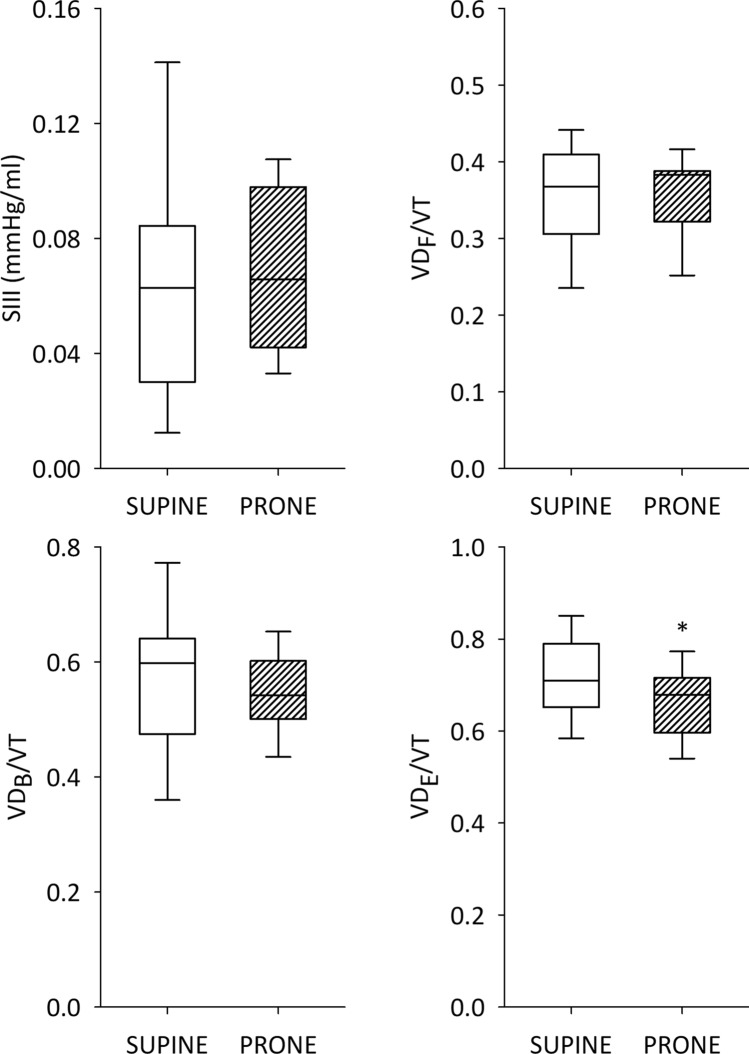
Severe COVID-19-related acute respiratory distress syndrome (C-ARDS) requires mechanical ventilation. While this intervention is often performed in the prone position to improve oxygenation, the underlying mechanisms responsible for the improvement in respiratory function during invasive ventilation and awake prone positioning in C-ARDS have not yet been elucidated. In this prospective observational trial, we evaluated the respiratory function of C-ARDS patients while in the supine and prone positions during invasive (n = 13) or non-invasive ventilation (n = 15). The primary endpoint was the positional change in lung regional aeration, assessed with electrical impedance tomography. Secondary endpoints included parameters of ventilation and oxygenation, volumetric capnography, respiratory system mechanics and intrapulmonary shunt fraction. In comparison to the supine position, the prone position significantly increased ventilation distribution in dorsal lung zones for patients under invasive ventilation (53.3 ± 18.3% vs. 43.8 ± 12.3%, percentage of dorsal lung aeration ± standard deviation in prone and supine positions, respectively; p = 0.014); whereas, regional aeration in both positions did not change during non-invasive ventilation (36.4 ± 11.4% vs. 33.7 ± 10.1%; p = 0.43). Prone positioning significantly improved the oxygenation both during invasive and non-invasive ventilation. For invasively ventilated patients reduced intrapulmonary shunt fraction, ventilation dead space and respiratory resistance were observed in the prone position. Oxygenation is improved during non-invasive and invasive ventilation with prone positioning in patients with C-ARDS. Different mechanisms may underly this benefit during these two ventilation modalities, driven by improved distribution of lung regional aeration, intrapulmonary shunt fraction and ventilation-perfusion matching. However, the differences in the severity of C-ARDS may have biased the sensitivity of electrical impedance tomography when comparing positional changes between the protocol groups.Trial registration: ClinicalTrials.gov (NCT04359407) and Registered 24 April 2020, https://clinicaltrials.gov/ct2/show/NCT04359407 .
严重的 COVID-19 相关急性呼吸窘迫综合征(C-ARDS)需要机械通气。虽然这种干预通常采用俯卧位以改善氧合,但在 ARDS 患者进行有创通气和清醒俯卧位时,导致呼吸功能改善的潜在机制尚未阐明。在这项前瞻性观察性试验中,我们评估了 C-ARDS 患者在有创(n = 13)或无创通气(n = 15)时仰卧位和俯卧位的呼吸功能。主要终点是使用电阻抗断层成像评估肺区域性通气的体位变化。次要终点包括通气和氧合参数、容积碳酸图、呼吸力学和肺内分流分数。与仰卧位相比,俯卧位显著增加了有创通气患者背部肺区的通气分布(53.3 ± 18.3%与 43.8 ± 12.3%,分别为俯卧位和仰卧位背部肺充气百分比±标准差;p = 0.014);而在无创通气时,两个位置的区域性通气均未改变(36.4 ± 11.4%与 33.7 ± 10.1%;p = 0.43)。俯卧位显著改善了有创和无创通气时的氧合。对于接受有创通气的患者,在俯卧位时观察到肺内分流分数、通气死腔和呼吸阻力降低。在 C-ARDS 患者中,俯卧位可改善无创和有创通气时的氧合。在这两种通气方式中,可能存在不同的机制导致俯卧位时区域性通气分布、肺内分流分数和通气-灌注匹配改善。然而,在比较方案组之间的体位变化时,严重程度不同的 ARDS 可能会影响电阻抗断层成像的敏感性。
ClinicalTrials.gov(NCT04359407),注册于 2020 年 4 月 24 日,https://clinicaltrials.gov/ct2/show/NCT04359407。