Enengl Sabine, Pecks Ulrich, Oppelt Peter, Stelzl Patrick, Trautner Philip Sebastian, Shebl Omar, Lamprecht Bernd, Longardt Ann Carolin, Eckmann-Scholz Christel, Keil Corinna, Mand Nadine, von Kaisenberg Constantin Sylvius, Jegen Magdalena, Doppler Stefan, Lastinger Julia
Department of Gynecology, Obstetrics, and Gynecological Endocrinology, Kepler University Hospital, Johannes Kepler University Linz, Linz, Austria.
Department of Obstetrics, Schleswig-Holstein University Hospital, Kiel, Germany.
Geburtshilfe Frauenheilkd. 2022 May 6;82(5):501-509. doi: 10.1055/a-1768-0415. eCollection 2022 May.
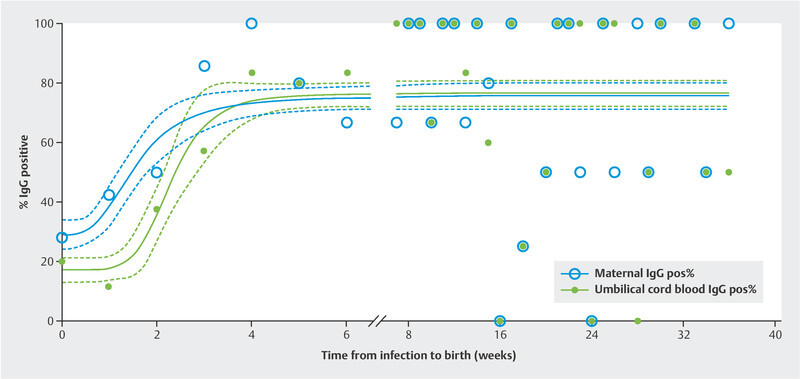
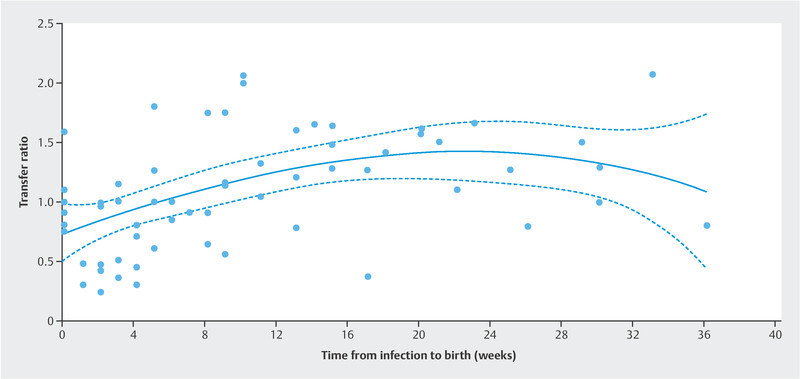
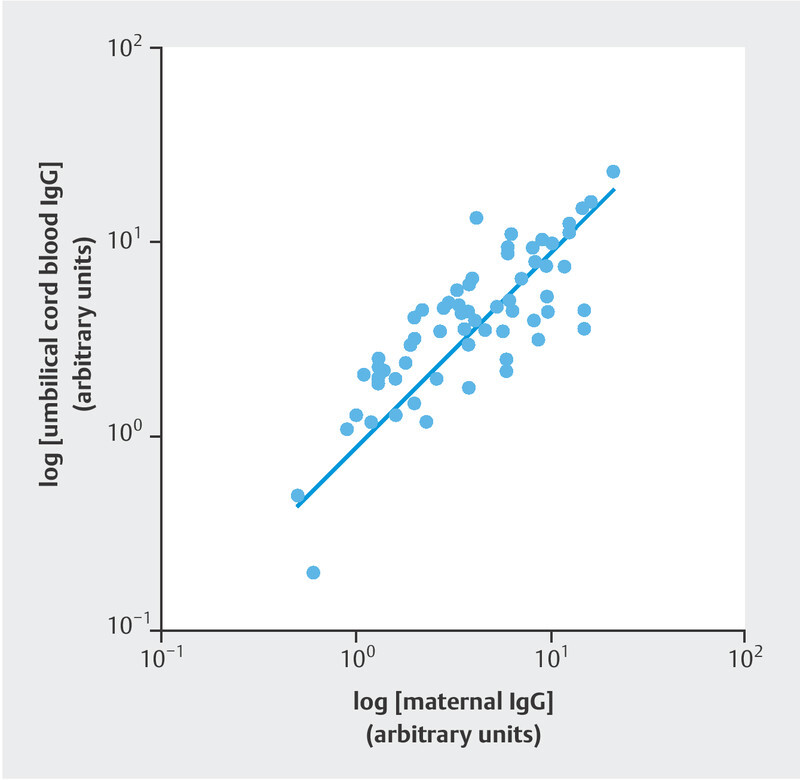
Awareness of SARS-CoV-2 infection in pregnant women and the potential risk for infection of their neonates is increasing. The aim of this study was to examine the immune status of affected women and evaluate the dynamics of placental antibody transfer. The study included 176 women with SARS-CoV-2 infection during pregnancy who delivered between April 2020 and December 2021 at eight obstetric maternity sites. Demographic data, maternal and neonatal characteristics were summarized. Antibody testing for IgA and IgG in maternal blood sera and umbilical cord samples was evaluated and IgG transfer ratios were calculated. Values were related to the time of infection during pregnancy and birth. The percentage of IgG positive women increased from 29.0% (95% CI 23.8 - 37.8) at presentation with a positive PCR test result to 75.7% (95% CI 71.6 - 79.8), the percentage of IgG positive umbilical cord blood samples increased from 17.1% (95% CI 13.0 - 21.3) to 76.4% (95% CI 72.2 - 80.7) at more than six weeks after infection. Regression lines differed significantly between maternal and fetal IgG responses (p < 0.0001). Newborns react with a latency of about one week; umbilical cord blood antibody concentrations are highly correlated with maternal concentration levels (ρ = 0.8042; p < 0.0001). IgG transplacental transfer ratios were dependent on infection-to-birth interval. Two of the umbilical cord blood samples tested positive for IgA. These findings confirm vertical SARS-CoV-2 transmission is rare; however, antibodies are transferred to the fetus soon after infection during pregnancy. Since transplacental antibody transfer might have a protective value for neonatal immunization this information may be helpful when counseling affected women.
孕妇感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)以及其新生儿感染的潜在风险正日益受到关注。本研究旨在检查受感染女性的免疫状态,并评估胎盘抗体转移的动态变化。该研究纳入了2020年4月至2021年12月期间在八个产科分娩地点分娩的176名孕期感染SARS-CoV-2的女性。总结了人口统计学数据、母婴特征。评估了母血血清和脐带样本中IgA和IgG的抗体检测情况,并计算了IgG转移率。这些值与孕期感染时间和分娩时间相关。IgG阳性女性的比例从PCR检测结果呈阳性时的29.0%(95%置信区间23.8 - 37.8)增加到75.7%(95%置信区间71.6 - 79.8),感染后六周以上时,IgG阳性脐带血样本的比例从17.1%(95%置信区间13.0 - 21.3)增加到76.4%(95%置信区间72.2 - 80.7)。母体和胎儿IgG反应的回归线差异显著(p < 0.0001)。新生儿的反应有大约一周的延迟;脐带血抗体浓度与母体浓度水平高度相关(ρ = 0.8042;p < 0.0001)。IgG经胎盘转移率取决于感染至分娩的间隔时间。两份脐带血样本的IgA检测呈阳性。这些发现证实SARS-CoV-2垂直传播很少见;然而,孕期感染后抗体很快就会转移到胎儿体内。由于经胎盘抗体转移可能对新生儿免疫有保护作用,这一信息在为受影响女性提供咨询时可能会有所帮助。