Department of Cardiac Surgery, The University of Tokyo, Tokyo, Japan.
Department of Therapeutic Strategy for Heart Failure, The University of Tokyo, Tokyo, Japan.
ESC Heart Fail. 2022 Aug;9(4):2491-2499. doi: 10.1002/ehf2.13951. Epub 2022 May 10.
The removal of left ventricular assist device (LVAD) after myocardial recovery can provide survival benefits with freedom from LVAD-associated complications. However, in the absence of standardization, the weaning evaluation and surgical strategy differ widely among centres. Therefore, we analysed the experiences of LVAD explantation with our protocol in dilated cardiomyopathy (DCM) patients and investigated the validity of our weaning evaluation and surgical strategy from the perspective of optimal long-term survival.
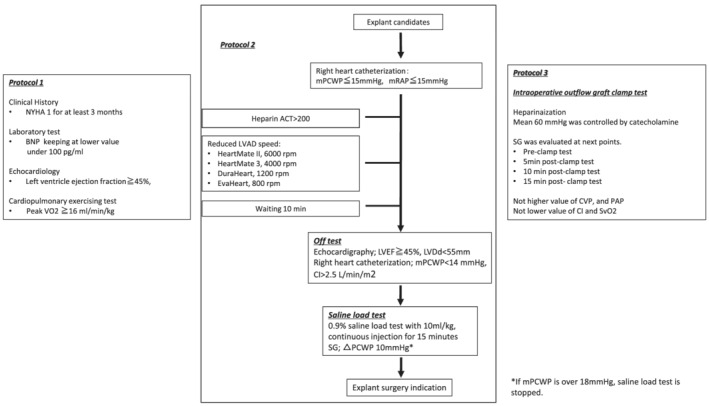
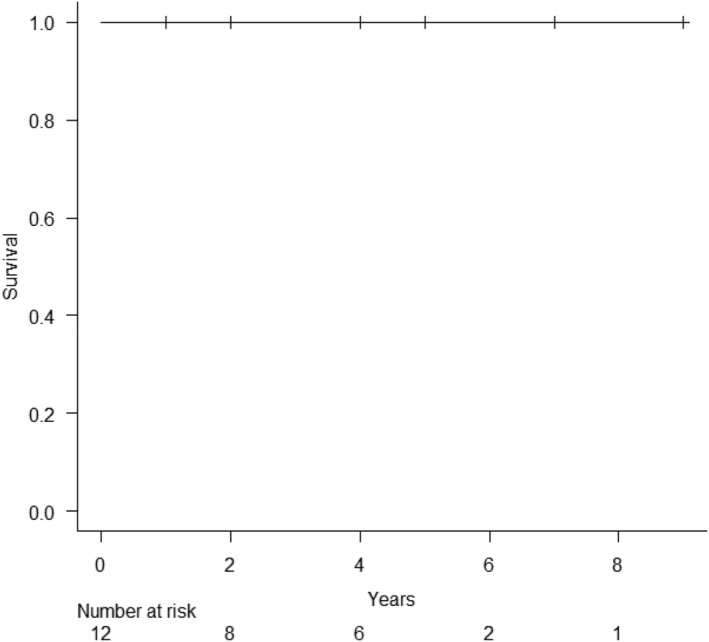
All LVAD explantation patients in our institution between May 2012 and May 2020 were enrolled. All patients were evaluated by our three-phase weaning assessment: (i) clinical stability with improved cardiac function under LVAD support; (ii) haemodynamic stability shown by ramp-loading and saline-loading test; (iii) intraoperative pump-off test. Explant surgery involved removal of the whole system including driveline, pump, sewing ring and outflow-graft, and closure of an apical hole. Intra-operative, peri-operative, and post-operative outcomes, including all-cause mortality and LVAD associated major complications, were retrospectively analysed. A total of 12 DCM patients (DuraHeart, n = 2; EVAHEART, n = 2; HeartMate II, n = 6; HeartMate 3, n = 2) had myocardial recovery after a median 10 months [interquartile range (IQR); 6.3-15 months] support and qualified for our LVAD explantation study protocol [median age: 37 y, IQR; 34-41 years; 83% men]. The median left ventricular ejection fraction was 20% (IQR; 12-23%) at LVAD-implantation and 54% (IQR: 45-55%) before LVAD explantation (P < 0.001). There were no perioperative complications and median ICU stay was 4 days (IQR; 2-4 days). All patients were discharged after a median of 24 days (IQR: 17-28 days) postoperatively. No patient suffered from any cardiac event (heart failure hospitalization, re-implantation of LVAD, or heart transplantation) at a median of 40 months (IQR: 17-58 months) follow up. All patients are alive with NYHA functional class 1 with preserved left ventricular function.
The evaluation of LVAD explant candidates by our weaning protocol was safe and effective. In the patients completing our protocol successfully, LVAD explantation is feasible and an excellent long-term cardiac event free-survival seems to be achieved.
左心室辅助装置(LVAD)在心功能恢复后移除可带来生存获益,同时避免与 LVAD 相关的并发症。然而,由于缺乏标准化,各中心之间的撤机评估和手术策略存在很大差异。因此,我们分析了我们的方案在扩张型心肌病(DCM)患者中 LVAD 移除的经验,并从最佳长期生存的角度探讨了我们的撤机评估和手术策略的有效性。
本研究纳入了 2012 年 5 月至 2020 年 5 月期间我院所有接受 LVAD 移除的患者。所有患者均采用我们的三阶段撤机评估:(i)LVAD 支持下心功能改善的临床稳定;(ii)通过斜坡加载和盐水加载试验显示血流动力学稳定;(iii)术中泵停试验。LVAD 移除手术包括移除整个系统,包括驱动线、泵、缝合环和流出道移植物,并闭合心尖孔。回顾性分析术中、围术期和术后结果,包括全因死亡率和与 LVAD 相关的主要并发症。
共有 12 例 DCM 患者(DuraHeart,n=2;EVAHEART,n=2;HeartMate II,n=6;HeartMate 3,n=2)在中位 10 个月(IQR:6.3-15 个月)的支持后出现心肌恢复,符合我们的 LVAD 移除研究方案[中位年龄:37 岁,IQR;34-41 岁;83%为男性]。LVAD 植入时的左心室射血分数中位数为 20%(IQR:12-23%),LVAD 移除前为 54%(IQR:45-55%)(P<0.001)。无围手术期并发症,中位 ICU 住院时间为 4 天(IQR:2-4 天)。所有患者在术后中位 24 天(IQR:17-28 天)出院。中位随访 40 个月(IQR:17-58 个月)时,无患者发生任何心脏事件(心力衰竭住院、LVAD 再植入或心脏移植)。所有患者均存活,NYHA 心功能分级 1 级,左心室功能正常。
通过我们的撤机方案评估 LVAD 移除候选者是安全有效的。在成功完成我们方案的患者中,LVAD 移除是可行的,并且似乎实现了极好的长期无心脏事件生存率。