University Health Network, Peter Munk Cardiac Centre, Division of Vascular Surgery, University of Toronto, Toronto, Ontario, Canada.
JAMA Netw Open. 2022 May 2;5(5):e2211336. doi: 10.1001/jamanetworkopen.2022.11336.
Sex differences in aortic surgery outcomes are commonly reported. However, data on ruptured abdominal aortic aneurysm (rAAA) repair outcomes in women vs men are limited.
To assess differences in perioperative and long-term mortality following rAAA repair in women vs men.
DESIGN, SETTING, AND PARTICIPANTS: A multicenter, retrospective cohort study was conducted using the Vascular Quality Initiative database, which prospectively captures information on patients who undergo vascular surgery across 796 academic and community hospitals in North America. All patients who underwent endovascular or open rAAA repair between January 1, 2003, and December 31, 2019, were included. Outcomes were assessed up to January 1, 2020.
Patient sex.
Demographic, clinical, and procedural characteristics were recorded, and differences between women vs men were assessed using independent t test and χ2 test. The primary outcomes were in-hospital and 8-year mortality. Associations between sex and outcomes were analyzed using univariable and multivariable logistic regression and Cox proportional hazards regression analysis.
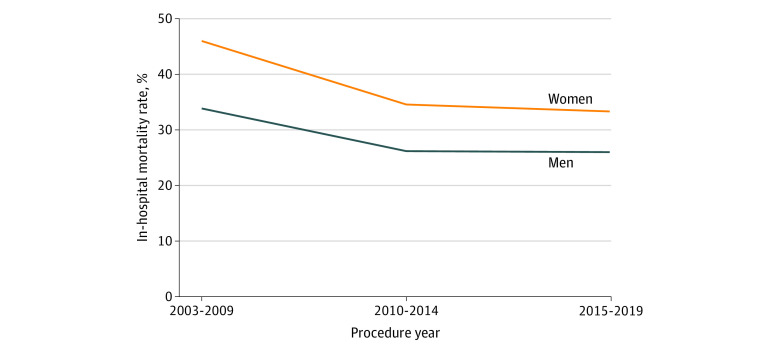
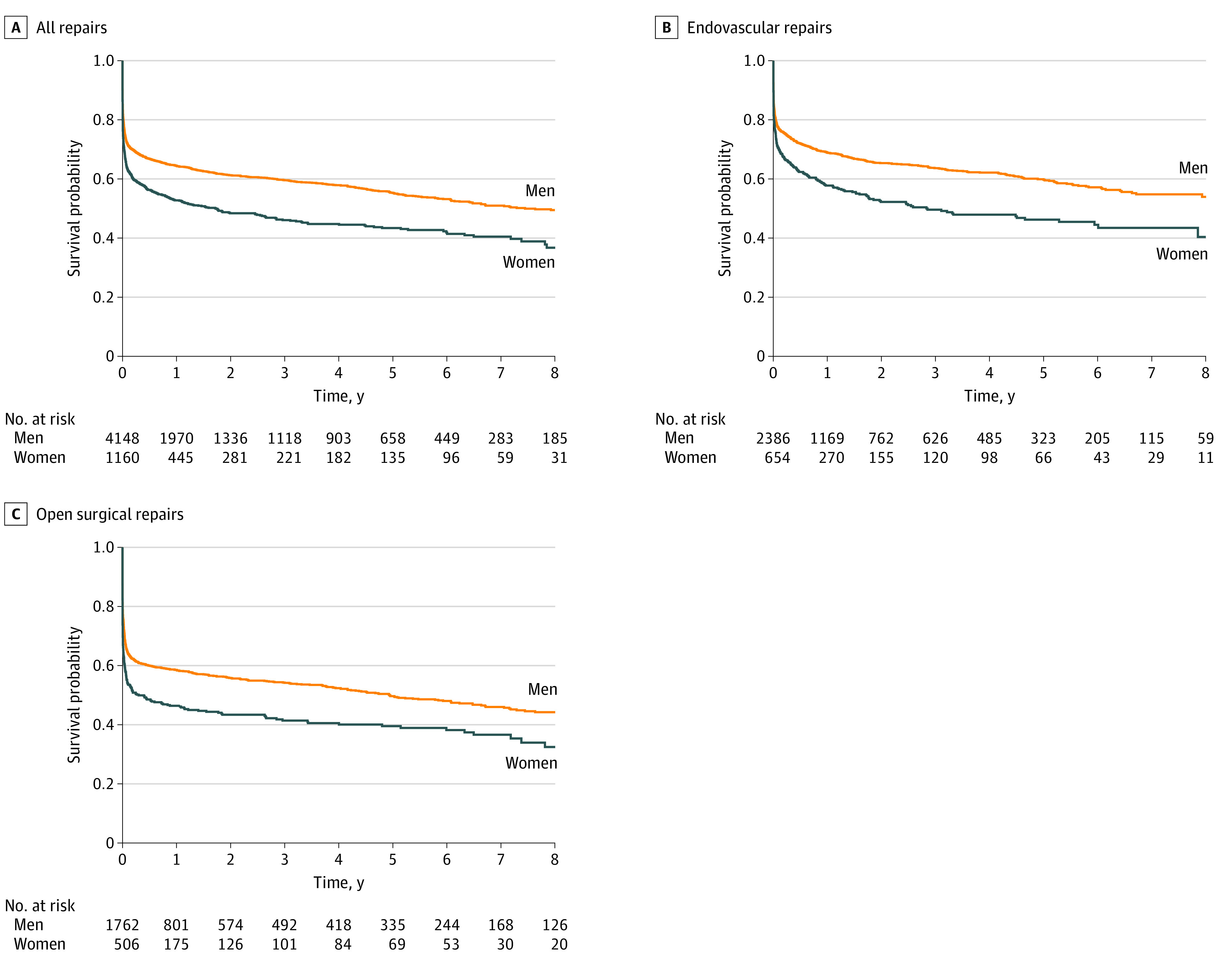
A total of 1160 (21.9%) women and 4148 (78.1%) men underwent rAAA repair during the study period. There was a similar proportion of endovascular repairs in women and men (654 [56.4%] vs 2386 [57.5%]). Women were older (mean [SD] age, 75.8 [9.3] vs 71.7 [9.6] years), more likely to have chronic kidney disease (718 [61.9%] vs 2184 [52.7%]), and presented with ruptured aneurysms of smaller diameters (mean [SD] 68 [18.2] vs 78 [30.2] mm). In-hospital mortality was higher in women (34.4% vs 26.6%; odds ratio, 1.44; 95% CI, 1.25-1.66), which persisted after adjusting for demographic, clinical, and procedural characteristics (adjusted odds ratio, 1.36; 95% CI, 1.12-1.66; P = .002). Eight-year survival was lower in women (36.7% vs 49.5%; hazard ratio, 1.25; 95% CI, 1.04-1.50; P = .02), which persisted when stratified by endovascular and open repair. This survival difference existed in both the US and Canada. Variables associated with long-term mortality in women included older age and chronic kidney disease.
Women who underwent rAAA repair had higher perioperative and 8-year mortality rates following both endovascular and open repair compared with men. Older age and higher rates of chronic kidney disease in women were associated with higher mortality rates. These findings suggest that future studies should assess the reasons for these disparities and whether opportunities exist to improve AAA care for women.
主动脉手术结果的性别差异通常是有报道的。然而,关于女性与男性腹主动脉瘤破裂(rAAA)修复结果的数据是有限的。
评估女性与男性 rAAA 修复后的围手术期和长期死亡率差异。
设计、设置和参与者:这是一项多中心、回顾性队列研究,使用血管质量倡议数据库进行,该数据库前瞻性地收集了北美 796 家学术和社区医院进行血管手术的患者信息。纳入 2003 年 1 月 1 日至 2019 年 12 月 31 日期间接受血管内或开放 rAAA 修复的所有患者。截至 2020 年 1 月 1 日评估结果。
患者性别。
记录了人口统计学、临床和程序特征,并使用独立 t 检验和 χ2 检验评估了女性与男性之间的差异。主要结局是院内和 8 年死亡率。使用单变量和多变量逻辑回归和 Cox 比例风险回归分析评估了性别与结局之间的关系。
在研究期间,共有 1160 名(21.9%)女性和 4148 名(78.1%)男性接受 rAAA 修复。女性和男性接受血管内修复的比例相似(654 [56.4%] 与 2386 [57.5%])。女性年龄较大(平均[标准差]年龄,75.8 [9.3] 岁与 71.7 [9.6] 岁),更可能患有慢性肾脏病(718 [61.9%] 与 2184 [52.7%]),并且破裂的动脉瘤直径较小(平均[标准差]直径,68 [18.2] 毫米与 78 [30.2] 毫米)。女性的院内死亡率更高(34.4% 与 26.6%;比值比,1.44;95%置信区间,1.25-1.66),调整人口统计学、临床和程序特征后仍然如此(调整比值比,1.36;95%置信区间,1.12-1.66;P=0.002)。女性 8 年生存率较低(36.7% 与 49.5%;风险比,1.25;95%置信区间,1.04-1.50;P=0.02),按血管内和开放修复分层后仍然如此。这种生存差异在美国和加拿大都存在。与女性长期死亡率相关的变量包括年龄较大和慢性肾脏病。
与男性相比,接受 rAAA 修复的女性围手术期和 8 年死亡率均较高。女性年龄较大和慢性肾脏病发生率较高与死亡率较高有关。这些发现表明,未来的研究应该评估这些差异的原因,以及是否有机会改善女性的 AAA 护理。