Cancer Prevention Research Program, Palindrome Liaisons Consultants, Montvale, NJ 07645-1559, USA.
Int J Mol Sci. 2022 Apr 27;23(9):4800. doi: 10.3390/ijms23094800.
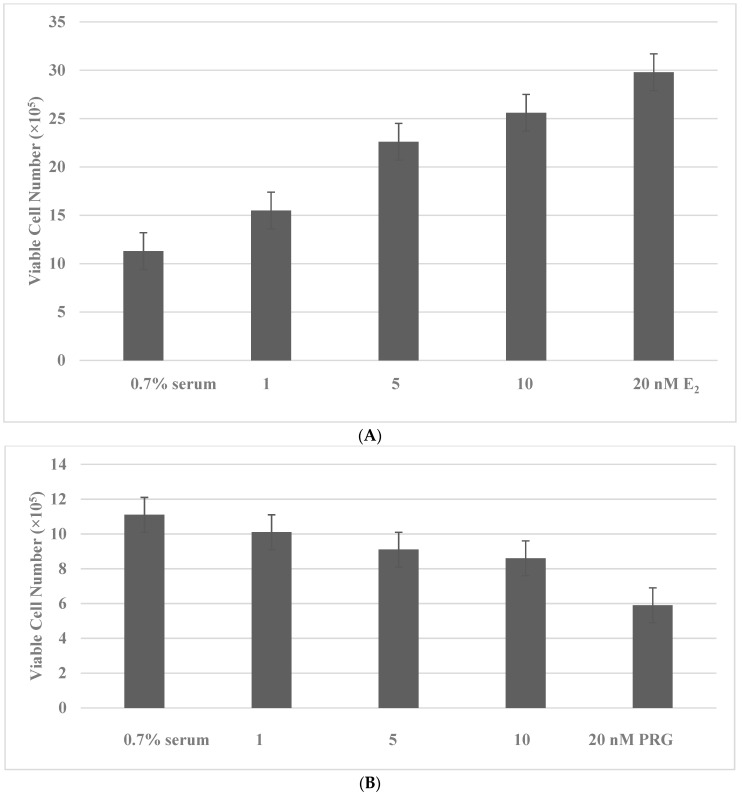
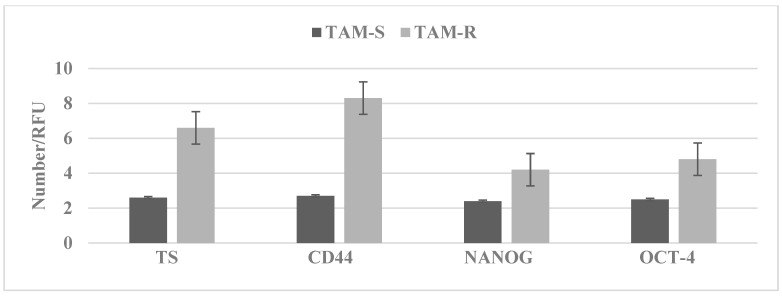
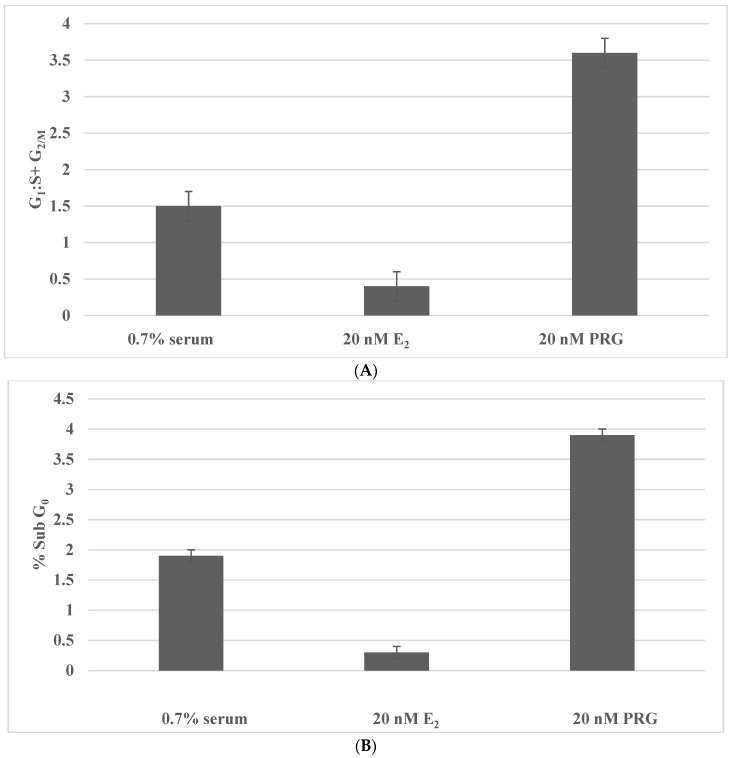
The growth modulating effects of the ovarian steroid hormones 17β-estradiol (E) and progesterone (PRG) on endocrine-responsive target tissues are well established. In hormone-receptor-positive breast cancer, E functions as a potent growth promoter, while the function of PRG is less defined. In the hormone-receptor-positive Luminal A and Luminal B molecular subtypes of clinical breast cancer, conventional endocrine therapy predominantly targets estrogen receptor function and estrogen biosynthesis and/or growth factor receptors. These therapeutic options are associated with systemic toxicity, acquired tumor resistance, and the emergence of drug-resistant cancer stem cells, facilitating the progression of therapy-resistant disease. The limitations of targeted endocrine therapy emphasize the identification of nontoxic testable alternatives. In the human breast, carcinoma-derived hormone-receptor-positive MCF-7 model treatment with E within the physiological concentration range of 1 nM to 20 nM induces progressive growth, upregulated cell cycle progression, and downregulated cellular apoptosis. In contrast, treatment with PRG at the equimolar concentration range exhibits dose-dependent growth inhibition, downregulated cell-cycle progression, and upregulated cellular apoptosis. Nontoxic nutritional herbs at their respective maximum cytostatic concentrations (IC) effectively increase the E metabolite ratio in favor of the anti-proliferative metabolite. The long-term exposure to the selective estrogen-receptor modulator tamoxifen selects a drug-resistant phenotype, exhibiting increased expressions of stem cell markers. The present review discusses the published evidence relevant to hormone metabolism, growth modulation by hormone metabolites, drug-resistant stem cells, and growth-inhibitory efficacy of nutritional herbs. Collectively, this evidence provides proof of the concept for future research directions that are focused on novel therapeutic options for endocrine therapy-resistant breast cancer that may operate via E- and/or PRG-mediated growth regulation.
卵巢甾体激素 17β-雌二醇(E)和孕酮(PRG)对内分泌反应性靶组织的生长调节作用已得到充分证实。在激素受体阳性乳腺癌中,E 作为一种有效的生长促进剂发挥作用,而 PRG 的作用则不太明确。在激素受体阳性的临床乳腺癌 Luminal A 和 Luminal B 分子亚型中,传统的内分泌治疗主要针对雌激素受体功能和雌激素生物合成和/或生长因子受体。这些治疗选择与全身毒性、获得性肿瘤耐药性以及耐药性癌症干细胞的出现有关,从而促进了治疗耐药性疾病的进展。靶向内分泌治疗的局限性强调了识别无毒可测试替代方案的重要性。在人乳腺中,癌源性激素受体阳性 MCF-7 模型在 1 nM 至 20 nM 的生理浓度范围内用 E 处理会诱导渐进性生长、上调细胞周期进程和下调细胞凋亡。相比之下,在等摩尔浓度范围内用 PRG 处理会表现出剂量依赖性的生长抑制、下调细胞周期进程和上调细胞凋亡。在各自最大细胞抑制浓度(IC)下的无毒营养草药有效地增加了 E 代谢物的比例,有利于抗增殖代谢物。长期暴露于选择性雌激素受体调节剂他莫昔芬会选择耐药表型,表现出干细胞标志物的表达增加。本综述讨论了与激素代谢、激素代谢物生长调节、耐药性干细胞以及营养草药生长抑制功效相关的已发表证据。总的来说,这些证据为未来的研究方向提供了概念验证,这些研究方向侧重于针对可能通过 E 和/或 PRG 介导的生长调节作用的内分泌治疗耐药性乳腺癌的新型治疗选择。