Al-Beltagi Mohammed, Bediwy Adel Salah, Saeed Nermin Kamal
Department of Pediatrics, Faculty of Medicine, Tanta University, Tanta 31511, Egypt.
Department of Chest Disease, Faculty of Medicine, Tanta University, Tanta 31527, Egypt.
World J Diabetes. 2022 Apr 15;13(4):282-307. doi: 10.4239/wjd.v13.i4.282.
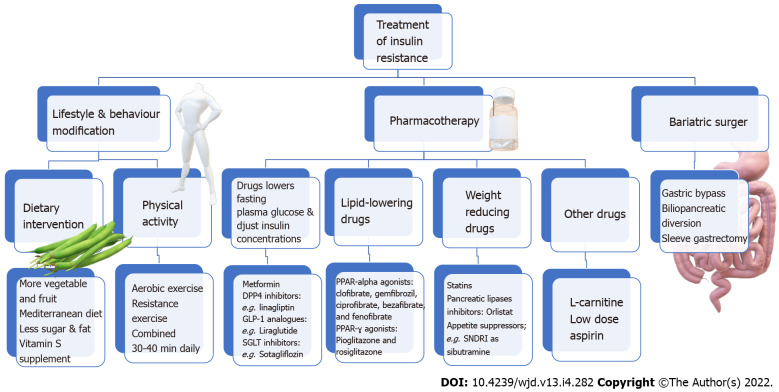
Insulin resistance (IR) is insulin failure in normal plasma levels to adequately stimulate glucose uptake by the peripheral tissues. IR is becoming more common in children and adolescents than before. There is a strong association between obesity in children and adolescents, IR, and the metabolic syndrome components. IR shows marked variation among different races, crucial to understanding the possible cardiovascular risk, specifically in high-risk races or ethnic groups. Genetic causes of IR include insulin receptor mutations, mutations that stimulate autoantibody production against insulin receptors, or mutations that induce the formation of abnormal glucose transporter 4 molecules or plasma cell membrane glycoprotein-1 molecules; all induce abnormal energy pathways and end with the development of IR. The parallel increase of IR syndrome with the dramatic increase in the rate of obesity among children in the last few decades indicates the importance of environmental factors in increasing the rate of IR. Most patients with IR do not develop diabetes mellitus (DM) type-II. However, IR is a crucial risk factor to develop DM type-II in children. Diagnostic standards for IR in children are not yet established due to various causes. Direct measures of insulin sensitivity include the hyperinsulinemia euglycemic glucose clamp and the insulin-suppression test. Minimal model analysis of frequently sampled intravenous glucose tolerance test and oral glucose tolerance test provide an indirect estimate of metabolic insulin sensitivity/resistance. The main aim of the treatment of IR in children is to prevent the progression of compensated IR to decompensated IR, enhance insulin sensitivity, and treat possible complications. There are three main lines for treatment: Lifestyle and behavior modification, pharmacotherapy, and surgery. This review will discuss the magnitude, implications, diagnosis, and treatment of IR in children.
胰岛素抵抗(IR)是指在正常血浆水平下胰岛素无法充分刺激外周组织摄取葡萄糖。如今,胰岛素抵抗在儿童和青少年中比以往更为常见。儿童和青少年肥胖、胰岛素抵抗以及代谢综合征各组分之间存在密切关联。胰岛素抵抗在不同种族间表现出显著差异,这对于理解潜在的心血管风险至关重要,尤其是在高危种族或族群中。胰岛素抵抗的遗传原因包括胰岛素受体突变、刺激针对胰岛素受体自身抗体产生的突变,或诱导异常葡萄糖转运蛋白4分子或浆细胞膜糖蛋白-1分子形成的突变;所有这些都会导致能量代谢途径异常,最终引发胰岛素抵抗。在过去几十年中,胰岛素抵抗综合征与儿童肥胖率的急剧上升同步增加,这表明环境因素在胰岛素抵抗发生率上升中具有重要作用。大多数胰岛素抵抗患者不会发展为2型糖尿病(DM)。然而,胰岛素抵抗是儿童患2型糖尿病的关键危险因素。由于多种原因,儿童胰岛素抵抗的诊断标准尚未确立。胰岛素敏感性的直接测量方法包括高胰岛素正葡萄糖钳夹技术和胰岛素抑制试验。对频繁采样的静脉葡萄糖耐量试验和口服葡萄糖耐量试验进行最小模型分析可间接估计代谢性胰岛素敏感性/抵抗。儿童胰岛素抵抗治疗的主要目标是防止代偿性胰岛素抵抗进展为失代偿性胰岛素抵抗,增强胰岛素敏感性,并治疗可能出现的并发症。治疗主要有三条途径:生活方式和行为改变、药物治疗及手术治疗。本综述将探讨儿童胰岛素抵抗的程度、影响、诊断和治疗。