Carson Joanne M, Hajarizadeh Behzad, Hanson Josh, O'Beirne James, Iser David, Read Phillip, Balcomb Anne, Davies Jane, Doyle Joseph S, Yee Jasmine, Martinello Marianne, Marks Philippa, Matthews Gail V, Dore Gregory J
The Kirby Institute, UNSW Sydney, Sydney, Australia.
Cairns and Hinterland Hospital and Health Service, Cairns, Australia.
J Viral Hepat. 2022 May 18;29(8):661-76. doi: 10.1111/jvh.13705.
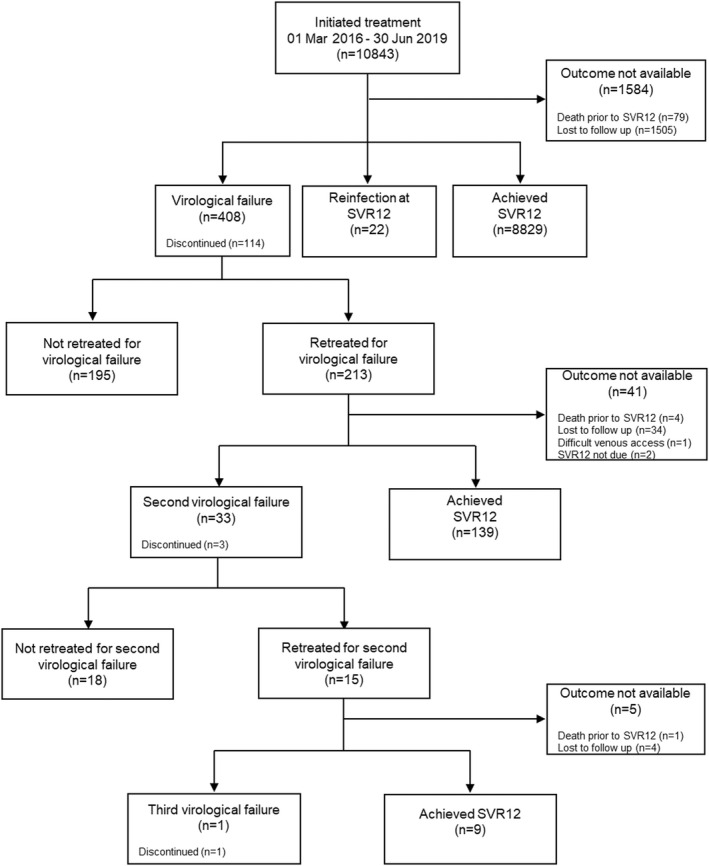
Virological failure occurs in a small proportion of people treated for hepatitis C virus (HCV) with direct-acting antiviral (DAA) therapies. This study assessed retreatment for virological failure in a large real-world cohort. REACH-C is an Australian observational study (n=10843) evaluating treatment outcomes of sequential DAA initiations across 33 health services between March 2016 to June 2019. Virological failure retreatment data were collected until October 2020. Of 408 people with virological failure (81% male; median age 53; 38% cirrhosis; 56% genotype 3), 213 (54%) were retreated once; 15 were retreated twice. A range of genotype specific and pangenotypic DAAs were used to retreat virological failure in primary (n=56) and tertiary (n=157) settings. Following sofosbuvir/velpatasvir/voxilaprevir availability in 2019, the proportion retreated in primary care increased from 21% to 40% and median time to retreatment initiation declined from 294 to 152 days. Per-protocol (PP) sustained virological response (SVR12) was similar for people retreated in primary and tertiary settings (80% vs 81%; p=1.000). In regression analysis, sofosbuvir/velpatasvir/voxilaprevir (vs. other regimens) significantly decreased likelihood of second virological failure (PP SVR12 88% vs. 77%; adjusted odds ratio [AOR] 0.29; 95%CI 0.11-0.81); cirrhosis increased likelihood (PP SVR12 69% vs. 91%; AOR 4.26; 95%CI 1.64-11.09). Indigenous Australians had lower likelihood of retreatment initiation (AOR 0.36; 95%CI 0.15-0.81). Treatment setting and prescriber type were not associated with retreatment initiation or outcome. Virological failure can be effectively retreated in primary care. Expanded access to simplified retreatment regimens through decentralised models may increase retreatment uptake and reduce HCV-related mortality.
一小部分接受丙型肝炎病毒(HCV)直接抗病毒药物(DAA)治疗的患者会出现病毒学失败。本研究评估了在一个大型真实世界队列中对病毒学失败患者的再次治疗情况。REACH-C是一项澳大利亚的观察性研究(n = 10843),评估了2016年3月至2019年6月期间33个医疗服务机构中连续启动DAA治疗的结果。收集病毒学失败再治疗数据至2020年10月。在408例病毒学失败患者中(81%为男性;中位年龄53岁;38%有肝硬化;56%为基因3型),213例(54%)接受了一次再次治疗;15例接受了两次再次治疗。一系列基因型特异性和泛基因型DAA被用于在初级(n = 56)和三级(n = 157)医疗机构中对病毒学失败患者进行再次治疗。2019年索磷布韦/维帕他韦/伏西瑞韦上市后,初级保健机构中接受再次治疗的比例从21%增至40%,再次治疗开始的中位时间从294天降至152天。初级和三级医疗机构中接受再次治疗的患者按方案(PP)持续病毒学应答(SVR12)相似(80%对81%;p = 1.000)。在回归分析中,索磷布韦/维帕他韦/伏西瑞韦(与其他方案相比)显著降低了第二次病毒学失败的可能性(PP SVR12为88%对77%;调整优势比[AOR] 0.29;95%CI 0.11 - 0.81);肝硬化增加了这种可能性(PP SVR12为69%对91%;AOR 4.26;95%CI 1.64 - 11.09)。澳大利亚原住民开始再次治疗的可能性较低(AOR 0.36;95%CI 0.15 - 0.81)。治疗机构和开处方者类型与再次治疗的开始或结果无关。病毒学失败在初级保健中可得到有效再次治疗。通过分散模式扩大对简化再治疗方案的获取可能会增加再次治疗的接受率并降低HCV相关死亡率。