Department of Global HIV, Hepatitis and STI Programmes, World Health Organization, Geneva, Switzerland.
Population Health Sciences, University of Bristol, Bristol, UK.
Lancet Glob Health. 2021 Apr;9(4):e431-e445. doi: 10.1016/S2214-109X(20)30505-2. Epub 2021 Feb 24.
Increasing access to hepatitis C virus (HCV) care and treatment will require simplified service delivery models. We aimed to evaluate the effects of decentralisation and integration of testing, care, and treatment with harm-reduction and other services, and task-shifting to non-specialists on outcomes across the HCV care continuum.
For this systematic review and meta-analysis, we searched PubMed, Embase, WHO Global Index Medicus, and conference abstracts for studies published between Jan 1, 2008, and Feb 20, 2018, that evaluated uptake of HCV testing, linkage to care, treatment, cure assessment, and sustained virological response at 12 weeks (SVR12) in people who inject drugs, people in prisons, people living with HIV, and the general population. Randomised controlled trials, non-randomised studies, and observational studies were eligible for inclusion. Studies with a sample size of ten or less for the largest denominator were excluded. Studies were categorised according to the level of decentralisation: full (testing and treatment at same site), partial (testing at decentralised site and referral elsewhere for treatment), or none. Task-shifting was categorised as treatment by specialists or non-specialists. Data on outcomes across the HCV care continuum (linkage to care, treatment uptake, and SVR12) were pooled using random-effects meta-analysis.
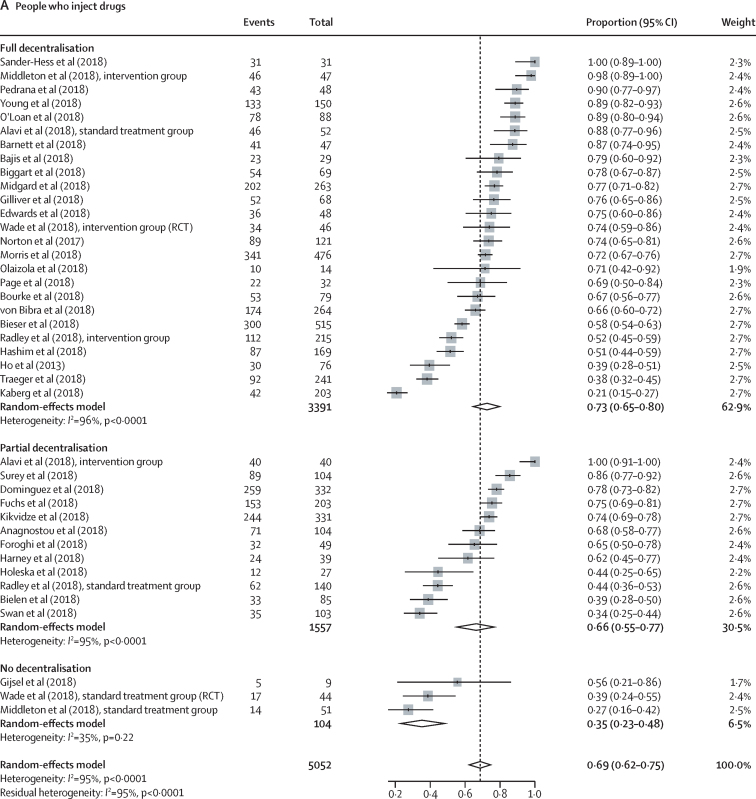
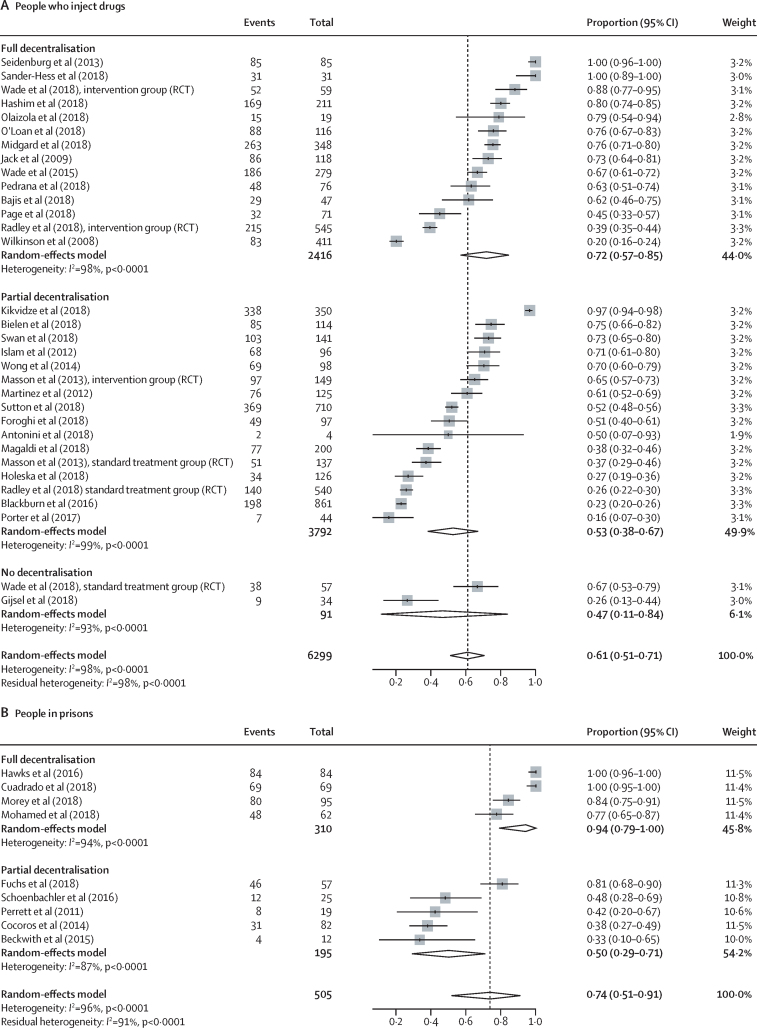
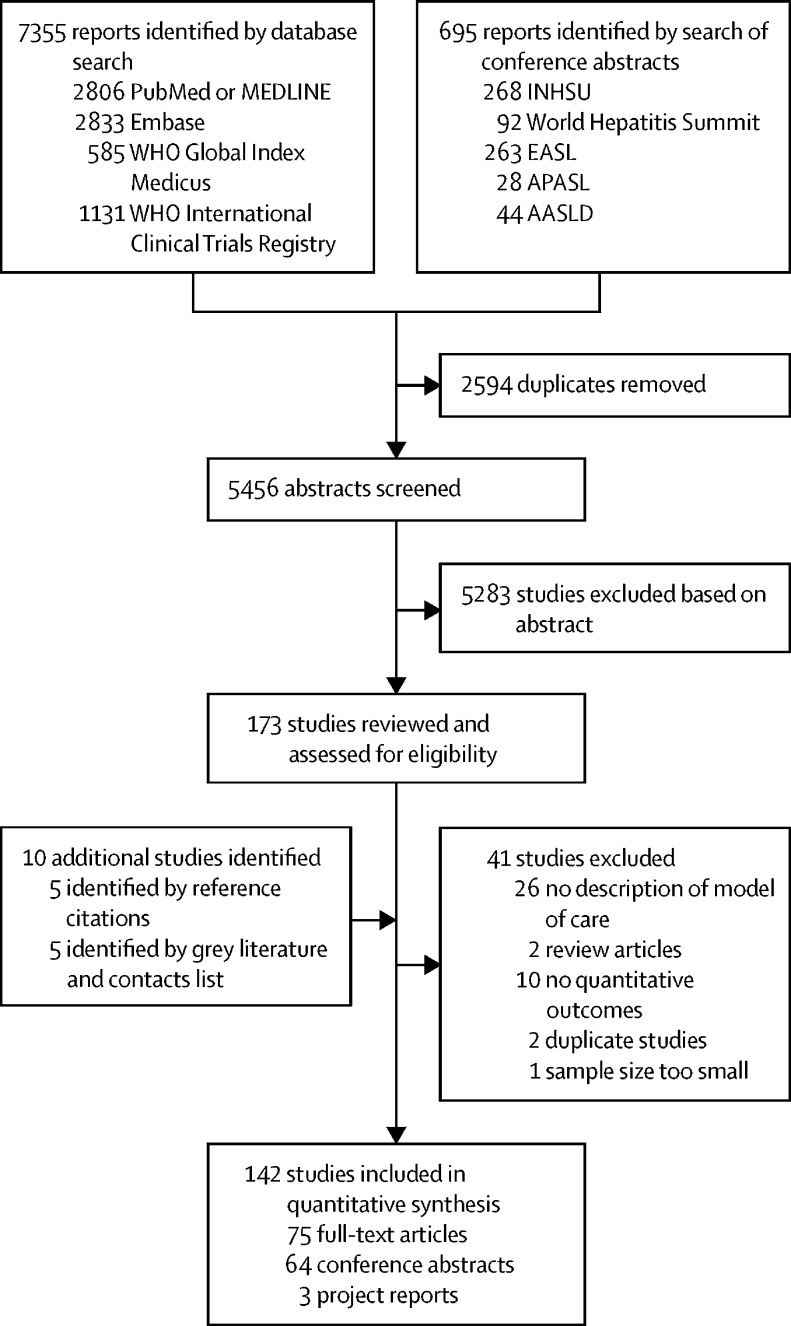
Our search identified 8050 reports, of which 132 met the eligibility criteria, and an additional ten reports were identified from reference citations and grey literature. Therefore, the final synthesis included 142 studies from 34 countries (20 [14%] studies from low-income and middle-income countries) and a total of 489 996 patients (239 446 [49%] from low-income and middle-income countries). Rates of linkage to care were higher with full decentralisation compared with partial or no decentralisation among people who inject drugs (full 72% [95% CI 57-85] vs partial 53% [38-67] vs none 47% [11-84]) and among people in prisons (full 94% [79-100] vs partial 50% [29-71]), although the CIs overlap for people who inject drugs. Similarly, treatment uptake was higher with full decentralisation compared with partial or no decentralisation (people who inject drugs: full 73% [65-80] vs partial 66% [55-77] vs none 35% [23-48]; people in prisons: full 72% [48-91] vs partial 39% [17-63]), although CIs overlap for full versus partial decentralisation. The results in the general population studies were more heterogeneous. SVR12 rates were high (≥90%) across different levels of decentralisation in all populations. Task-shifting of care and treatment to a non-specialist was associated with similar SVR12 rates to treatment delivered by specialists. There was a severe or critical risk of bias for 46% of studies, and heterogeneity across studies tended to be very high (I>90%).
Decentralisation and integration of HCV care to harm-reduction sites or primary care showed some evidence of improved access to testing, linkage to care, and treatment, and task-shifting of care and treatment to non-specialists was associated with similarly high cure rates to care delivered by specialists, across a range of populations and settings. These findings provide support for the adoption of decentralisation and task-shifting to non-specialists in national HCV programmes.
Unitaid.
增加丙型肝炎病毒(HCV)治疗和护理的机会将需要简化服务交付模式。我们旨在评估检测、护理和治疗与减少伤害以及其他服务的去中心化和整合,以及向非专家的任务转移对整个 HCV 护理连续体的结果的影响。
在这项系统综述和荟萃分析中,我们在 PubMed、Embase、世界卫生组织全球索引医学和会议摘要中搜索了 2008 年 1 月 1 日至 2018 年 2 月 20 日期间发表的研究,这些研究评估了在注射毒品者、监狱中的人、感染艾滋病毒的人和一般人群中,HCV 检测、护理、治疗、疗效评估和 12 周持续病毒学应答(SVR12)的检测、治疗和治疗的接受率。随机对照试验、非随机研究和观察性研究符合纳入标准。最大分母为十或更少的样本量的研究被排除在外。研究根据去中心化的程度进行分类:完全(在同一地点进行检测和治疗)、部分(在去中心化地点进行检测,并转介到其他地方进行治疗)或无。任务转移被归类为专家或非专家进行治疗。使用随机效应荟萃分析汇总了整个 HCV 护理连续体(护理、治疗接受和 SVR12)的结果数据。
我们的搜索确定了 8050 份报告,其中 132 份符合资格标准,另外还从参考文献和灰色文献中确定了 10 份报告。因此,最终综合包括来自 34 个国家的 142 项研究(20 项来自低收入和中等收入国家)和总共 489996 名患者(239446 名来自低收入和中等收入国家)。与部分或无去中心化相比,在注射毒品者(完全 72%[57-85]与部分 53%[38-67]与无 47%[11-84])和监狱中的人中,完全去中心化与部分或无去中心化相比,与护理的联系率更高,尽管在注射毒品者中 CI 重叠。同样,与部分或无去中心化相比,完全去中心化与治疗的接受率更高(注射毒品者:完全 73%[65-80]与部分 66%[55-77]与无 35%[23-48];监狱中的人:完全 72%[48-91]与部分 39%[17-63]),尽管完全与部分去中心化的 CI 重叠。一般人群研究的结果更为混杂。在所有人群中,不同程度的去中心化都有较高的 SVR12 率(≥90%)。将护理和治疗任务转移给非专家与由专家提供的护理和治疗的 SVR12 率相似。46%的研究存在严重或关键的偏倚风险,且研究之间的异质性往往非常高(I>90%)。
HCV 护理的去中心化和整合到减少伤害的场所或初级保健中心表明,在一定程度上改善了检测、护理和治疗的机会,将护理和治疗任务转移给非专家与由专家提供的护理和治疗的治愈率相似,这在一系列人群和环境中都得到了证实。这些发现为国家 HCV 方案采用去中心化和向非专家转移提供了支持。
联合国艾滋病规划署。