Iio Shunya, Hozaka Yuto, Tanoue Kiyonori, Idichi Tetsuya, Fukuda Kousuke, Nakashima Taiki, Yasudome Ryutaro, Yamasaki Yoichi, Kawasaki Yota, Arigami Takaaki, Nakajo Akihiro, Higashi Michiyo, Mataki Yuko, Kurahara Hiroshi, Ohtsuka Takao
Department of Digestive Surgery, Breast and Thyroid Surgery, Graduate School of Medical and Dental Sciences, Kagoshima University, 8-35-1, Sakuragaoka, Kagoshima, 890-8520, Japan.
Department of Pathology, Graduate School of Medical and Dental Sciences, Kagoshima University, 8-35-1 Sakuragaoka, Kagoshima, 890-8544, Japan.
Surg Case Rep. 2022 May 19;8(1):101. doi: 10.1186/s40792-022-01452-3.
Locoregional recurrence and metastasis to the liver, peritoneum, and lung are the most common recurrent patterns of pancreatic ductal adenocarcinoma (PDAC) after radical resection. Recurrence in the abdominal wall is extremely rare. Herein, we report our experience with a patient who had recurrent PDAC in the abdominal wall with long-term survival by means of multidisciplinary therapy.
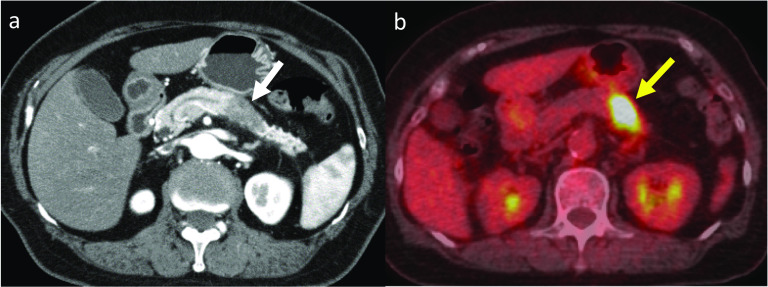
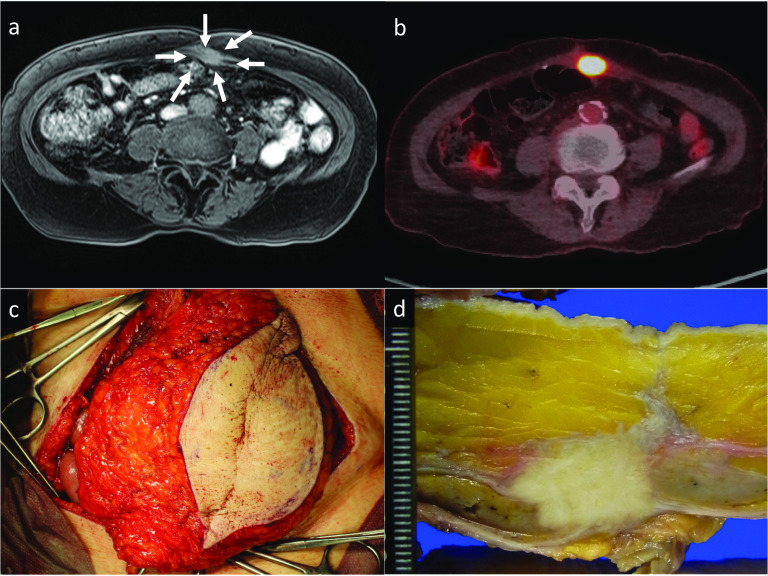
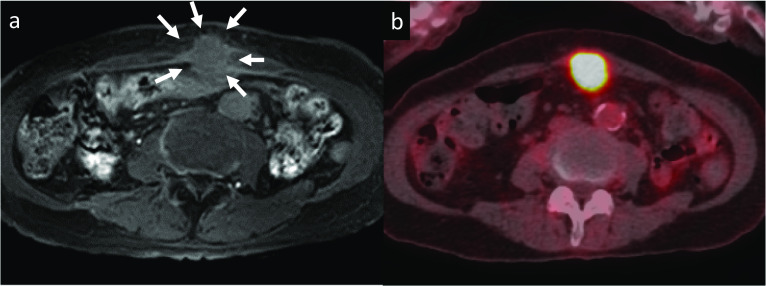
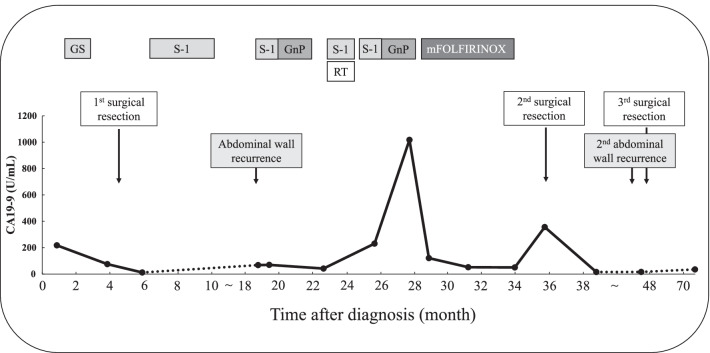
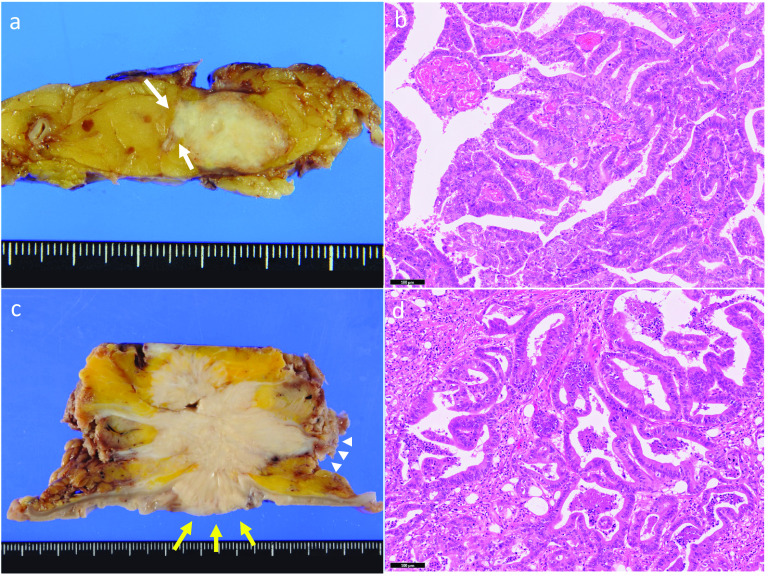
A 76-year-old Japanese woman was diagnosed with resectable pancreatic tail cancer. She underwent distal pancreatectomy with regional lymphadenectomy after two cycles of gemcitabine plus S-1 as neoadjuvant therapy. She also received eight cycles of S-1 as adjuvant chemotherapy. Approximately 14 months after the initial surgery, imaging examinations identified a mass suggesting recurrence in the abdominal wall at the middle wound that involved the transverse colon. After two cycles of gemcitabine plus nab-paclitaxel, chemoradiotherapy (S-1 plus 45 Gy) and seven cycles of modified FOLFIRINOX (5-fluorouracil/leucovorin, irinotecan, and oxaliplatin) were administered. The patient did not develop any new recurrent lesions during chemotherapy and chemoradiotherapy. Therefore, the recurrent lesion in the abdominal wall and the involved transverse colon were resected. We confirmed the lack of peritoneal dissemination during surgery. Pathological examination revealed that the resected lesion was metastasis of primary PDAC, and the surgical margin was 1 mm. However, re-recurrence localized in the abdominal wall was detected 9 months later. The re-recurrent lesion was diagnosed as local recurrence of the first recurrent lesion. We performed a second resection of the abdominal wall using a femoral myocutaneous flap to achieve sufficient surgical margin. The pathological findings of the resected specimen were the same as those of the previous specimens, and the resection margin was negative. The patient's postoperative course was uneventful. Seven years after the initial surgery and 3 years and 7 months after the third surgery, the patient is alive with no signs of recurrence.
Long-term survival could be achieved by radical resection with sufficient surgical margins for recurrence of PDAC in the abdominal wall if new other recurrent lesions, including peritoneal dissemination, are prevented through chemotherapy.
局部区域复发以及肝、腹膜和肺转移是胰腺导管腺癌(PDAC)根治性切除术后最常见的复发模式。腹壁复发极为罕见。在此,我们报告一例通过多学科治疗实现长期生存的腹壁复发性PDAC患者的经验。
一名76岁的日本女性被诊断为可切除的胰尾癌。在接受两个周期的吉西他滨加S-1作为新辅助治疗后,她接受了远端胰腺切除术及区域淋巴结清扫术。她还接受了八个周期的S-1作为辅助化疗。初次手术后约14个月,影像学检查发现中腹部伤口处腹壁有一肿块提示复发,累及横结肠。在接受两个周期的吉西他滨加纳米白蛋白结合型紫杉醇治疗后,给予了同步放化疗(S-1加45 Gy)以及七个周期的改良FOLFIRINOX方案(5-氟尿嘧啶/亚叶酸钙、伊立替康和奥沙利铂)。患者在化疗和同步放化疗期间未出现任何新的复发病灶。因此,切除了腹壁的复发病灶及受累的横结肠。术中确认无腹膜播散。病理检查显示切除的病灶为原发性PDAC转移灶,手术切缘为1毫米。然而,9个月后在腹壁检测到再次复发。再次复发病灶被诊断为首次复发病灶的局部复发。我们使用股薄肌皮瓣对腹壁进行了二次切除以获得足够的手术切缘。切除标本的病理结果与之前的标本相同,切缘阴性。患者术后恢复顺利。初次手术后7年以及第三次手术后3年7个月,患者仍存活,无复发迹象。
如果通过化疗预防包括腹膜播散在内的其他新的复发病灶,对腹壁复发性PDAC进行具有足够手术切缘的根治性切除可实现长期生存。