Division of Geriatrics, University of California, San Francisco, 490 Illinois Street, Floor 08, San Francisco, CA, 94158, USA.
Geriatrics, Palliative and Extended Care Service Line, San Francisco Veterans Affairs Health Care System, San Francisco, CA, USA.
BMC Geriatr. 2022 May 18;22(1):434. doi: 10.1186/s12877-022-03126-z.
Electronic health record (EHR) prediction models may be easier to use in busy clinical settings since EHR data can be auto-populated into models. This study assessed whether adding functional status and/or Medicare claims data (which are often not available in EHRs) improves the accuracy of a previously developed Veterans Affairs (VA) EHR-based mortality index.
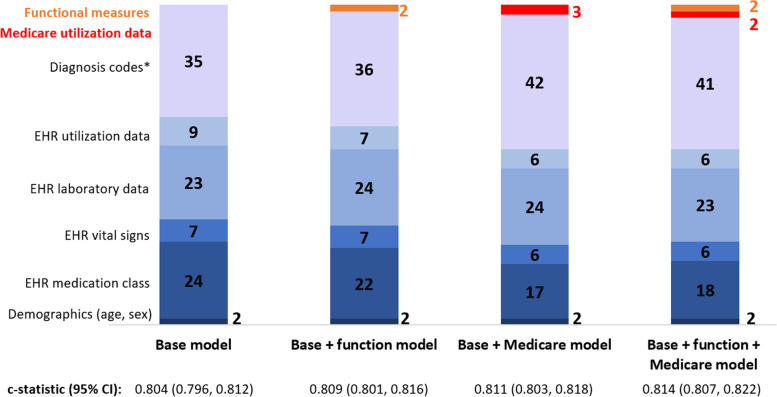
This was a retrospective cohort study of veterans aged 75 years and older enrolled in VA primary care clinics followed from January 2014 to April 2020 (n = 62,014). We randomly split participants into development (n = 49,612) and validation (n = 12,402) cohorts. The primary outcome was all-cause mortality. We performed logistic regression with backward stepwise selection to develop a 100-predictor base model using 854 EHR candidate variables, including demographics, laboratory values, medications, healthcare utilization, diagnosis codes, and vitals. We incorporated functional measures in a base + function model by adding activities of daily living (range 0-5) and instrumental activities of daily living (range 0-7) scores. Medicare data, including healthcare utilization (e.g., emergency department visits, hospitalizations) and diagnosis codes, were incorporated in a base + Medicare model. A base + function + Medicare model included all data elements. We assessed model performance with the c-statistic, reclassification metrics, fraction of new information provided, and calibration plots.
In the overall cohort, mean age was 82.6 years and 98.6% were male. At the end of follow-up, 30,263 participants (48.8%) had died. The base model c-statistic was 0.809 (95% CI 0.805-0.812) in the development cohort and 0.804 (95% CI 0.796-0.812) in the validation cohort. Validation cohort c-statistics for the base + function, base + Medicare, and base + function + Medicare models were 0.809 (95% CI 0.801-0.816), 0.811 (95% CI 0.803-0.818), and 0.814 (95% CI 0.807-0.822), respectively. Adding functional status and Medicare data resulted in similarly small improvements among other model performance measures. All models showed excellent calibration.
Incorporation of functional status and Medicare data into a VA EHR-based mortality index led to small but likely clinically insignificant improvements in model performance.
电子健康记录 (EHR) 预测模型在繁忙的临床环境中可能更容易使用,因为 EHR 数据可以自动填充到模型中。本研究评估了在之前开发的基于退伍军人事务部 (VA) 的 EHR 的死亡率指数中添加功能状态和/或医疗保险索赔数据(通常在 EHR 中不可用)是否可以提高准确性。
这是一项回顾性队列研究,纳入了年龄在 75 岁及以上、在 VA 初级保健诊所登记并在 2014 年 1 月至 2020 年 4 月期间随访的退伍军人(n=62014)。我们将参与者随机分为开发(n=49612)和验证(n=12402)队列。主要结局是全因死亡率。我们使用逻辑回归进行向后逐步选择,使用 854 个 EHR 候选变量(包括人口统计学、实验室值、药物、医疗保健利用、诊断代码和生命体征)开发了一个包含 100 个预测因素的基础模型。我们通过添加日常生活活动(范围 0-5)和工具性日常生活活动(范围 0-7)评分,在基础+功能模型中纳入了功能测量。在基础+医疗保险模型中纳入了医疗保险数据,包括医疗保健利用(例如急诊就诊、住院)和诊断代码。基础+功能+医疗保险模型包括所有数据元素。我们使用 c 统计量、重新分类指标、提供的新信息分数和校准图来评估模型性能。
在整个队列中,平均年龄为 82.6 岁,98.6%为男性。随访结束时,30263 名参与者(48.8%)死亡。基础模型的 c 统计量在开发队列中为 0.809(95%CI 0.805-0.812),在验证队列中为 0.804(95%CI 0.796-0.812)。验证队列中基础+功能、基础+医疗保险和基础+功能+医疗保险模型的 c 统计量分别为 0.809(95%CI 0.801-0.816)、0.811(95%CI 0.803-0.818)和 0.814(95%CI 0.807-0.822)。纳入功能状态和医疗保险数据对其他模型性能指标的改善作用相似。所有模型均显示出极好的校准度。
将功能状态和医疗保险数据纳入 VA 基于 EHR 的死亡率指数,可导致模型性能的微小但可能无临床意义的改善。