Section of Cancer Genomics, Genetics Branch, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA.
Department of General, Visceral and Pediatric Surgery, University Medical Center, Göttingen, Germany.
Br J Cancer. 2022 Sep;127(4):766-775. doi: 10.1038/s41416-022-01842-2. Epub 2022 May 21.
Preoperative (neoadjuvant) chemoradiotherapy (CRT) and total mesorectal excision is the standard treatment for rectal cancer patients (UICC stage II/III). Up to one-third of patients treated with CRT achieve a pathological complete response (pCR). These patients could be spared from surgery and its associated morbidity and mortality, and assigned to a "watch and wait" strategy. However, reliably identifying pCR based on clinical or imaging parameters remains challenging.
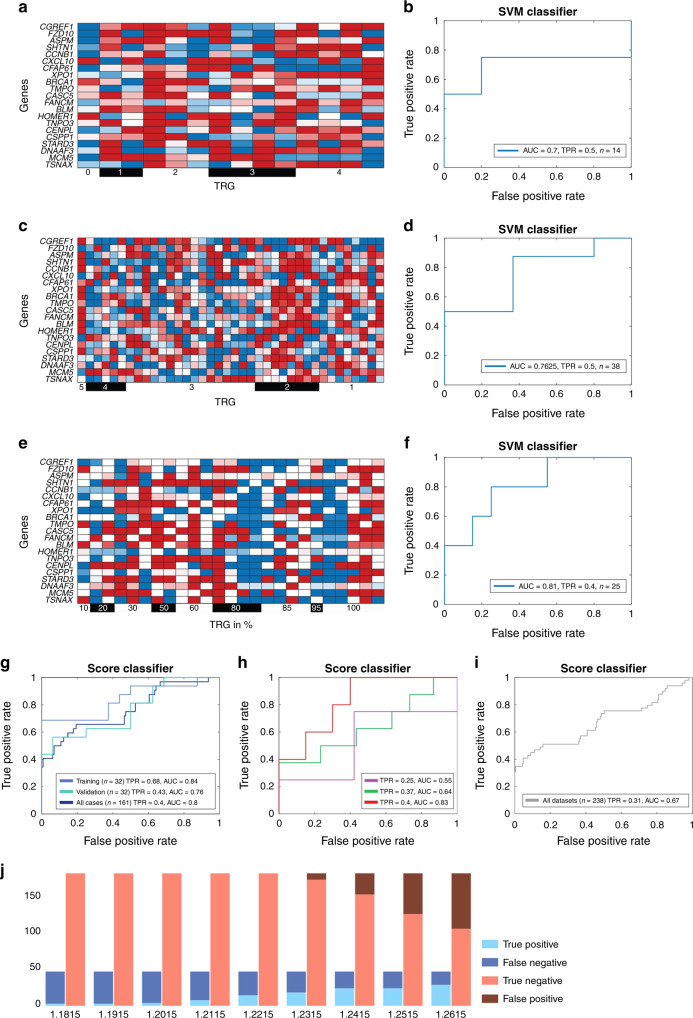
We generated gene-expression profiles of 175 patients with locally advanced rectal cancer enrolled in the CAO/ARO/AIO-94 and -04 trials. One hundred and sixty-one samples were used for building, training and validating a predictor of pCR using a machine learning algorithm. The performance of the classifier was validated in three independent cohorts, comprising 76 patients from (i) the CAO/ARO/AIO-94 and -04 trials (n = 14), (ii) a publicly available dataset (n = 38) and (iii) in 24 prospectively collected samples from the TransValid A trial.
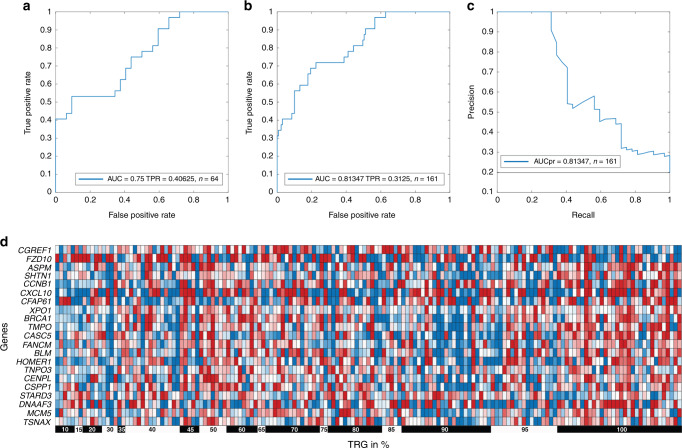
A 21-transcript signature yielded the best classification of pCR in 161 patients (Sensitivity: 0.31; AUC: 0.81), when not allowing misclassification of non-complete-responders (False-positive rate = 0). The classifier remained robust when applied to three independent datasets (n = 76).
The classifier can identify >1/3 of rectal cancer patients with a pCR while never classifying patients with an incomplete response as having pCR. Importantly, we could validate this finding in three independent datasets, including a prospectively collected cohort. Therefore, this classifier could help select rectal cancer patients for a "watch and wait" strategy.
Forgoing surgery with its associated side effects could be an option for rectal cancer patients if the prediction of a pathological complete response (pCR) after preoperative chemoradiotherapy would be possible. Based on gene-expression profiles of 161 patients a classifier was developed and validated in three independent datasets (n = 76), identifying over 1/3 of patients with pCR, while never misclassifying a non-complete-responder. Therefore, the classifier can identify patients suited for "watch and wait".
术前(新辅助)放化疗(CRT)和全直肠系膜切除术是局部晚期直肠癌患者(UICC 分期 II/III 期)的标准治疗方法。多达三分之一接受 CRT 治疗的患者可获得病理完全缓解(pCR)。这些患者可以免于手术及其相关的发病率和死亡率,并被分配到“观察等待”策略。然而,基于临床或影像学参数可靠地识别 pCR 仍然具有挑战性。
我们生成了 175 名局部晚期直肠癌患者的基因表达谱,这些患者参与了 CAO/ARO/AIO-94 和 -04 试验。161 个样本用于构建、训练和验证使用机器学习算法预测 pCR 的预测因子。该分类器的性能在三个独立队列中进行了验证,这些队列包括:(i)CAO/ARO/AIO-94 和 -04 试验中的 76 名患者(n=14),(ii)一个公开可用的数据集(n=38)和(iii)TransValid A 试验中 24 个前瞻性收集的样本。
在 161 名患者中,21 个转录本特征可最好地分类 pCR(敏感性:0.31;AUC:0.81),且不允许将非完全缓解者错误分类为 pCR(假阳性率=0)。当应用于三个独立数据集(n=76)时,该分类器仍然稳健。
该分类器可以识别超过三分之一的 pCR 局部晚期直肠癌患者,而不会将不完全缓解者错误分类为 pCR。重要的是,我们可以在三个独立的数据集(包括一个前瞻性收集的队列)中验证这一发现。因此,该分类器可以帮助选择适合“观察等待”策略的直肠癌患者。
翻译后的文本与原文在意思上是一致的,用词准确,语法正确。