Department of Surgical Oncology and Breast Surgery, the First Affiliated Hospital of China Medical University, Shenyang, China.
Department of Pathology, the First Affiliated Hospital of China Medical University, Shenyang, China.
Cancer Med. 2022 Dec;11(24):4767-4783. doi: 10.1002/cam4.4804. Epub 2022 May 22.
Mucinous breast cancer (MBC) is a rare disease, and patients with lymph node metastasis (LNM) have a poor prognosis. We aimed to explore the predictive factors of LNM and to construct a nomogram for predicting the risk of LNM and to identify the suitable axillary surgery for patients with diverse risks.
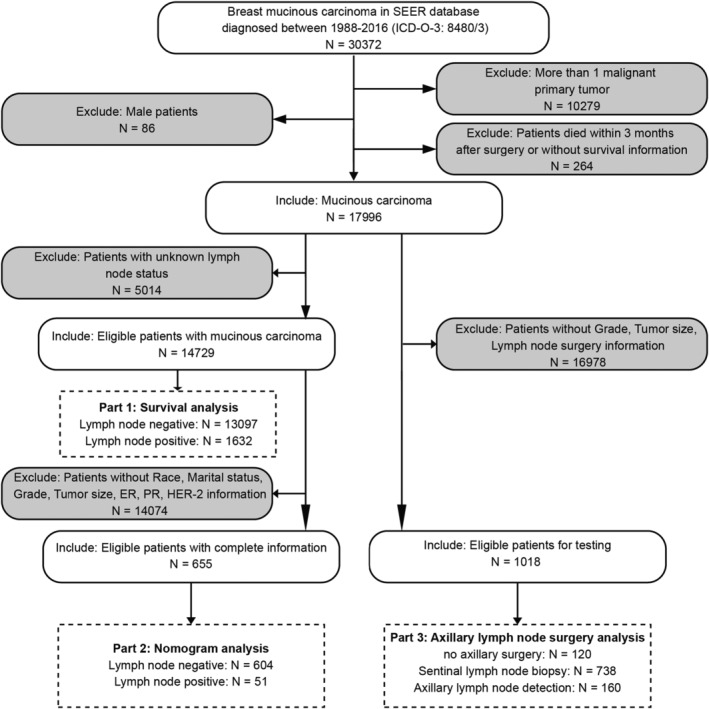
Data were extracted from the Surveillance, Epidemiology, and End Results (SEER) database. Chi-square and rank-sum tests were used to analyze the differences between groups. Survival analysis was performed with Kaplan-Meier curves and log-rank tests. Independent factor identification and nomogram construction were performed with logistic regression analysis. The nomogram was qualified with a discrimination and calibration plot. Propensity score matching was performed to balance the disparities between groups.
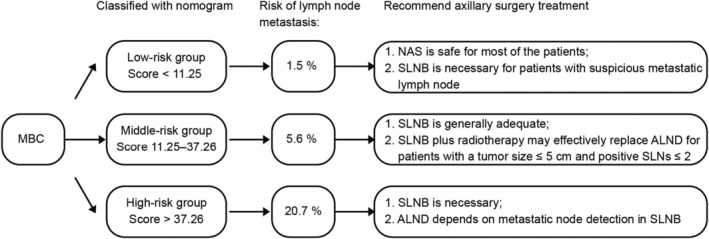
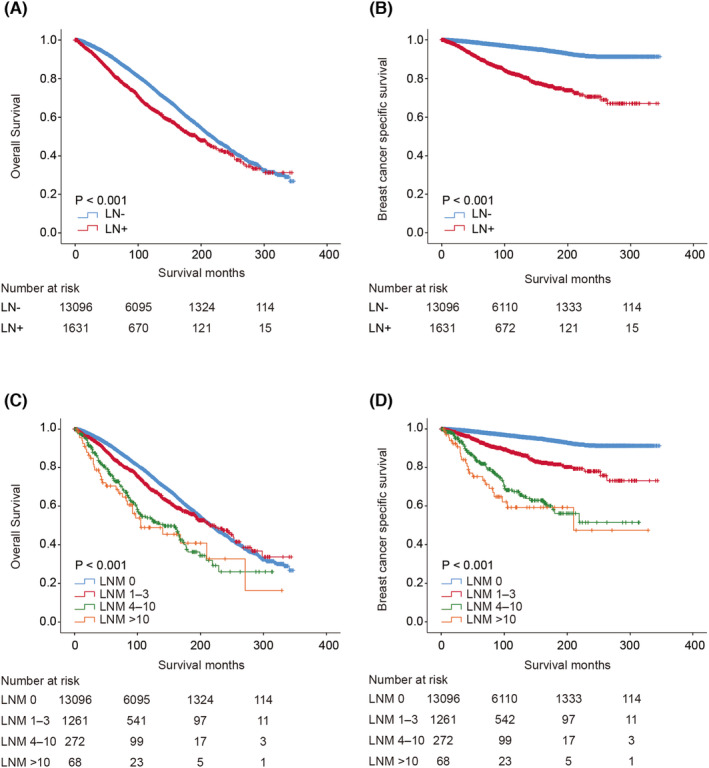
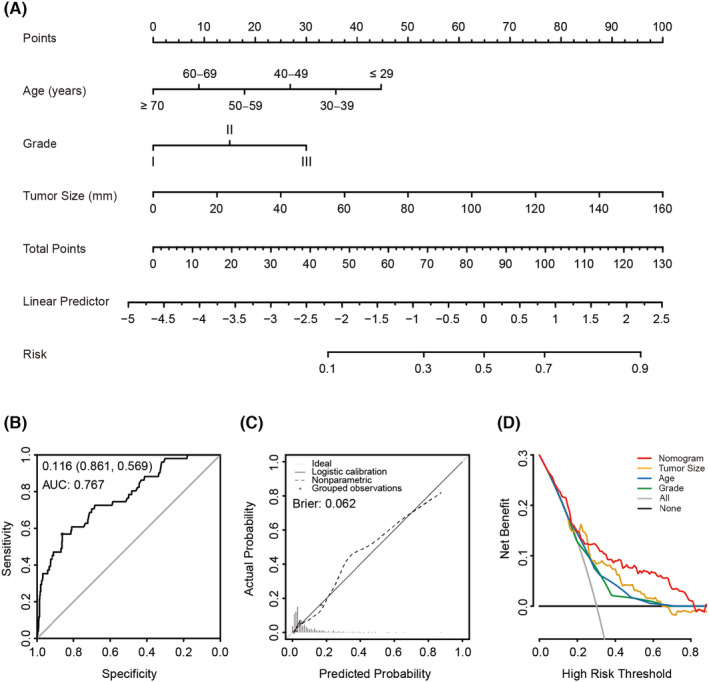
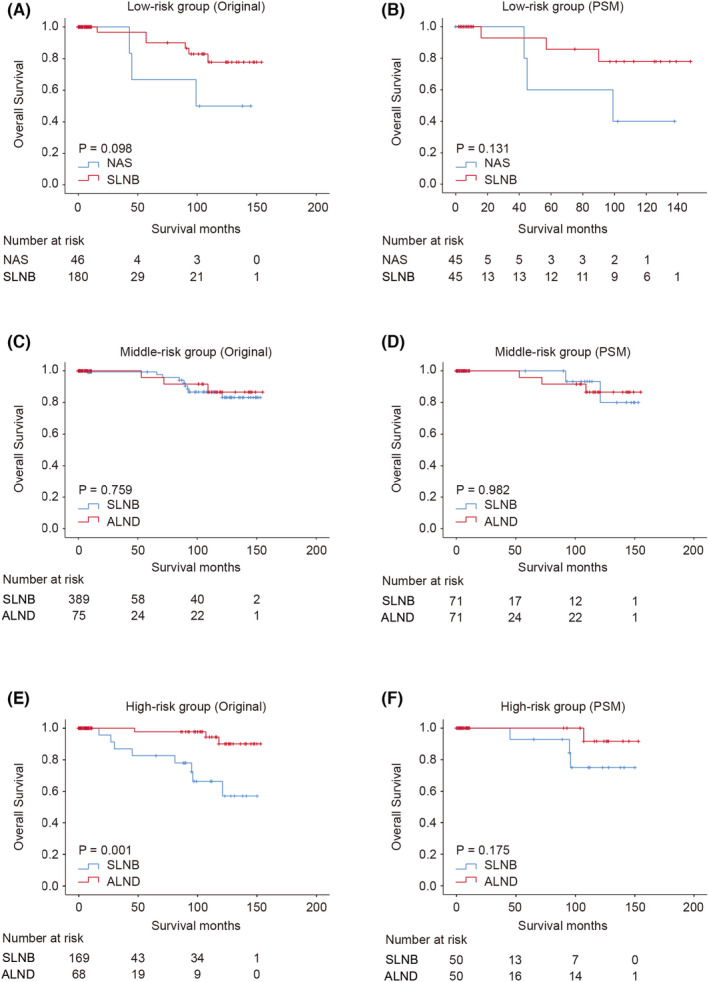
Patients with metastatic lymph nodes have a worse prognosis. Univariate and multivariate analyses indicated that tumor size, grade, and age were independent risk factors for LNM. The nomogram constructed with these three factors can predict the risk of LNM with high accuracy (AUC: 0.767, 95% CI: 0.697-0.838) and good calibration. Based on the nomogram, a risk classification system satisfactorily stratified the patients into 3 groups with diverse risks of LNM. In the low-risk group, there were no significant differences between sentinel lymph node biopsy and no axillary surgery. In the middle- and high-risk groups, both SLNB and axillary lymph node dissection were superior to no axillary surgery, with similar survival benefits.
The nomogram based on tumor size, grade, and age could conveniently and accurately predict the risk of LNM in MBC and assist clinicians in optimizing surgical strategies.
黏液性乳腺癌(MBC)是一种罕见的疾病,发生淋巴结转移(LNM)的患者预后较差。我们旨在探讨 LNM 的预测因素,构建预测 LNM 风险的列线图,并为不同风险患者确定合适的腋窝手术方式。
从监测、流行病学和最终结果(SEER)数据库中提取数据。使用卡方检验和秩和检验分析组间差异。采用 Kaplan-Meier 曲线和对数秩检验进行生存分析。使用 logistic 回归分析进行独立因素识别和列线图构建。通过鉴别和校准图对列线图进行验证。采用倾向评分匹配法平衡组间差异。
发生淋巴结转移的患者预后较差。单因素和多因素分析表明肿瘤大小、分级和年龄是 LNM 的独立危险因素。由这三个因素构建的列线图可以准确预测 LNM 的风险(AUC:0.767,95%CI:0.697-0.838),且校准度良好。基于列线图构建的风险分类系统可将患者满意地分为 3 组,每组 LNM 风险不同。在低危组中,前哨淋巴结活检与无腋窝手术之间无显著差异。在中高危组中,SLNB 和腋窝淋巴结清扫均优于无腋窝手术,且生存获益相似。
基于肿瘤大小、分级和年龄的列线图可方便、准确地预测 MBC 患者 LNM 的风险,有助于临床医生优化手术策略。