Eguchi Hiroi, Kakiuchi Toshihiko, Nishi Masanori, Kojima-Ishii Kanako, Nishiyama Kei, Koga Yuhki, Matsuo Muneaki
Department of Pediatrics, Faculty of Medicine, Saga University, Saga, Japan.
Department of Pediatrics, Graduate School of Medicine Sciences, Kyushu University, Fukuoka, Japan.
Front Pediatr. 2022 May 6;10:898531. doi: 10.3389/fped.2022.898531. eCollection 2022.
Juvenile myelomonocytic leukemia (JMML), which is predominantly found in infants, is a clonal abnormality of pluripotent hematopoietic stem cells and presents with the symptoms of both myeloproliferative tumors and myelodysplastic syndromes. Estimates have shown that ~20 cases of JMML occur annually in Japan. Ornithine transcarbamylase deficiency (OTCD), the most common among all urea cycle disorders (UCDs), occurs in 1 of 80,000 people in Japan.
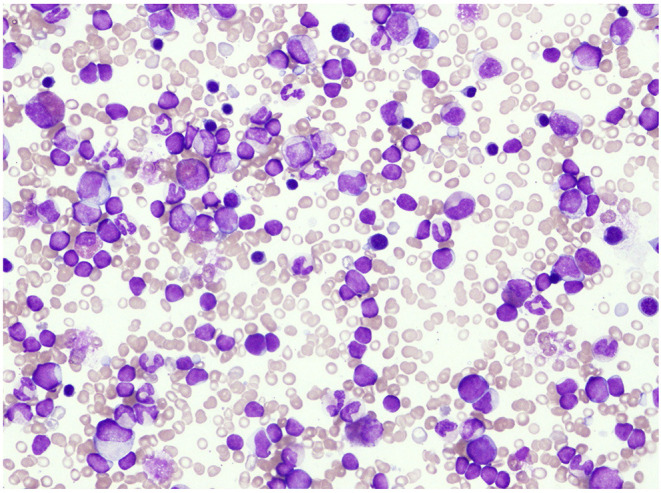
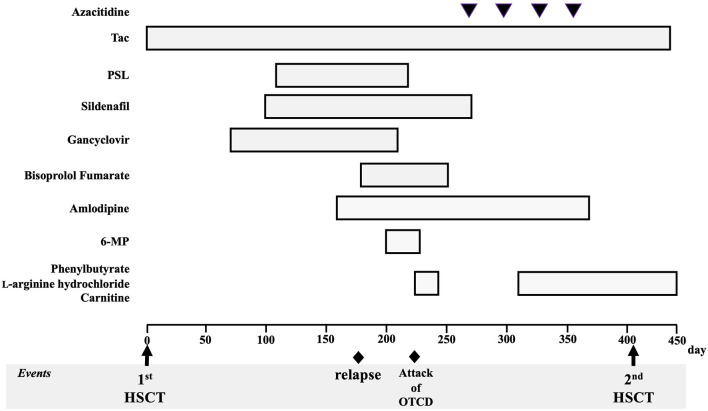
A 10-month-old infant who had fever, vomiting, and diarrhea for 2 days was referred to our hospital for the following abnormalities in blood tests: white blood cell count, 48,200/μL; hemoglobin, 9.0 g/dL; and platelet count, 135,000/μL. Bone marrow examination showed a nucleated cell count of 396,000/mm and blast cell count of 5.0%, as well as decreased mature granulocyte count and slightly myeloperoxidase stain-negative blasts but no monoclonal cell proliferation on May-Giemsa staining. Colony assay showed the proliferation of spontaneous colony and high sensitivity to granulocyte-macrophage colony-stimulating factor. Genetic analysis of peripheral blood mononuclear cells showed that the patient was positive for neuroblastoma RAS () mutation. The patient was ultimately diagnosed with JMML. Approximately 170 days after his first hematopoietic stem cell transplantation (HSCT), the patient's JMML relapsed. Shortly after the recurrence, nausea, vomiting, hyperventilation, and decreased vitality were observed, followed by a decrease in the level of consciousness. The patient's ammonia level was 472 μmol/L. A test for seven different genetic mutations for the UCD showed the presence of c. 119G>A (amino acid change p. Arg40His). As such, late-onset OTCD was added to his diagnosis. Administration of sodium phenylacetate, l-arginine hydrochloride, and carnitine was continued following the diagnosis of OTCD, after which hyperammonemia was not observed. Regarding JMML relapse, HSCT was performed on day 405 after the first transplantation.
Hyperammonemia should be considered a differential diagnosis when unexplained and non-specific symptoms occur during the treatment of hematologic malignancies. Patients should be tested for UCD as a cause of hyperammonemia, and treatment for hyperammonemia should be continued until the cause is identified. The patient shows normal developmental progress, has an intact neurological status, and has not experienced another hyperammonemia attack. His JMML has remained in remission for over 3 years.
青少年粒单核细胞白血病(JMML)主要见于婴儿,是一种多能造血干细胞的克隆性异常,具有骨髓增殖性肿瘤和骨髓增生异常综合征的症状。据估计,日本每年约有20例JMML病例发生。鸟氨酸转氨甲酰酶缺乏症(OTCD)是所有尿素循环障碍(UCD)中最常见的一种,在日本每80000人中就有1例发病。
一名10个月大的婴儿因发热、呕吐和腹泻2天,因血液检查出现以下异常被转诊至我院:白细胞计数48200/μL;血红蛋白9.0 g/dL;血小板计数135000/μL。骨髓检查显示有核细胞计数为396000/mm,原始细胞计数为5.0%,成熟粒细胞计数减少,髓过氧化物酶染色略呈阴性的原始细胞,但May-Giemsa染色未见单克隆细胞增殖。集落测定显示自发集落增殖及对粒细胞-巨噬细胞集落刺激因子高度敏感。外周血单个核细胞的基因分析显示该患者神经母细胞瘤RAS()突变呈阳性。该患者最终被诊断为JMML。在他首次造血干细胞移植(HSCT)约170天后,患者的JMML复发。复发后不久,观察到恶心、呕吐、呼吸急促和活力下降,随后意识水平降低。患者的氨水平为472μmol/L。对UCD的七种不同基因突变检测显示存在c.119G>A(氨基酸变化p.Arg40His)。因此,迟发性OTCD被追加到他的诊断中。在诊断OTCD后继续给予苯乙酸钠、盐酸l-精氨酸和肉碱治疗,此后未观察到高氨血症。关于JMML复发,在首次移植后第405天进行了HSCT。
在血液系统恶性肿瘤治疗期间出现无法解释的非特异性症状时,应考虑高氨血症的鉴别诊断。应对患者进行UCD检测以确定高氨血症的病因,并且应持续进行高氨血症治疗直至确定病因。该患者发育进程正常,神经状态完好,未再次发生高氨血症发作。他的JMML已缓解超过3年。