Oncology Hematology and Cell Therapy Department, French National Agency for Safety of Medicines and Health Products ANSM, Saint-Denis, France.
Department of Pharmacy, Centre hospitalo-universitaire Hôpital Henri Mondor Assistance Publique des Hôpitaux de Paris, Créteil, France.
Int J Cancer. 2022 Oct 15;151(8):1345-1354. doi: 10.1002/ijc.34129. Epub 2022 Jul 7.
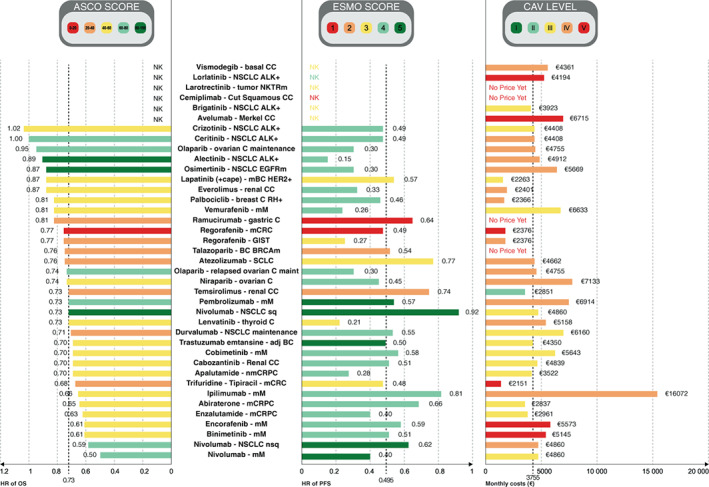
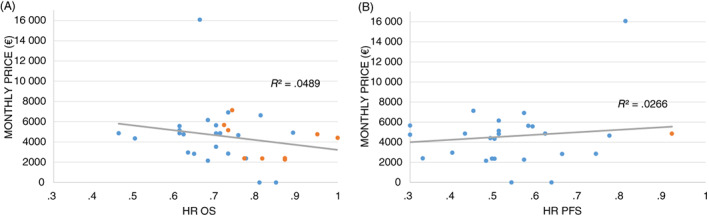
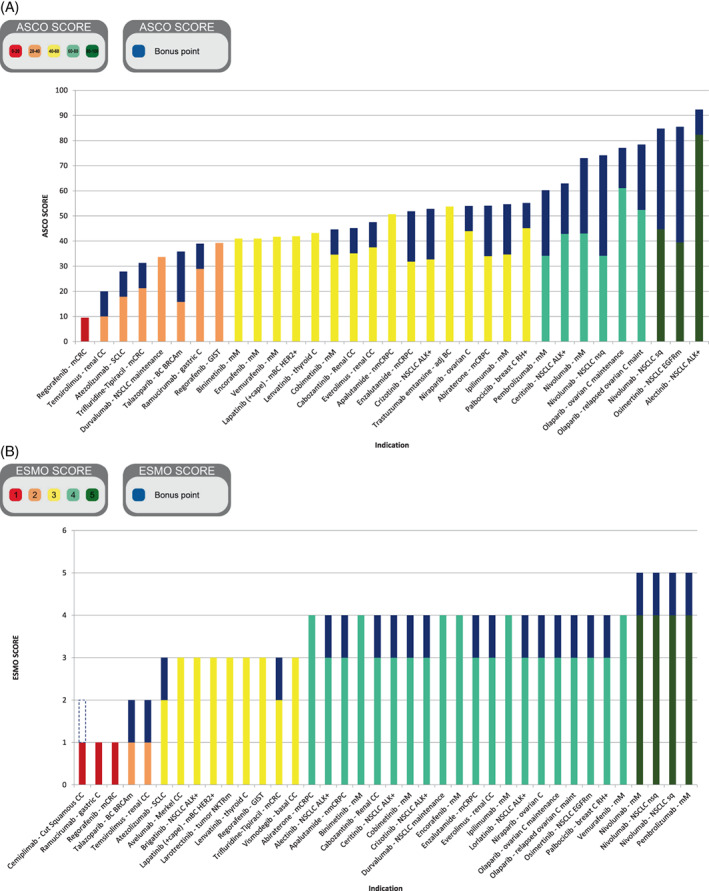
Decisions on market authorization (MA) and reimbursement have different durations across countries because of health technology assessment (HTA) procedures and negotiations between manufacturers and national authorities. To overcome this delay, France has implemented a Temporary Authorization for Use (ATU) program that allows early access to drugs before MA, in order to treat patients with unmet medical needs. The objectives of our study were to establish the added therapeutic benefit (ATB) of ATUs for solid tumors and to investigate the correlations between three tools evaluating ATB and survival outcomes and drug costs. Data on ATUs granted from January 2009 to December 2019 to treat solid tumors were analyzed. An assessment of their ATB was conducted using the American Society of Clinical Oncology-Value Framework (ASCO-VF), the European Society for Medical Oncology-Magnitude Clinical Benefit Scale (ESMO-MCBS) and the French HTA criterion, clinical added value (CAV). The latter score determines reimbursement and national market access. Thirty-five drugs in 39 indications were granted ATUs. All of them obtained MA and derived a clinical benefit to be reimbursed by the Social Security. Twenty-eight (71.8%) had CAV compared to preexisting therapies. 24/38 (63.2%) had a 4-5 ESMO-MCBS score and 19/33 (57.6%) had an ASCO-VF score over 45. No correlations were found between cost, PFS, OS, CAV and ASCO-VF score, while high ESMO-MCBS scores were correlated to OS. In conclusion, many patients were treated with innovations before MA thanks to ATU, although there are discrepancies between ATB scales, hence the importance of international collaboration in the evaluation of innovative therapies.
药品的上市许可和报销决策在不同国家的持续时间有所不同,这是由于卫生技术评估(HTA)程序以及制造商与国家主管部门之间的谈判。为了克服这种延迟,法国实施了临时使用授权(ATU)计划,允许在上市许可之前提前获得药物,以治疗有未满足医疗需求的患者。我们的研究目的是确定 ATU 在实体瘤方面的附加治疗效益(ATB),并研究评估 ATB 的三种工具与生存结果和药物成本之间的相关性。分析了从 2009 年 1 月至 2019 年 12 月授予治疗实体瘤的 ATU 数据。使用美国临床肿瘤学会-价值框架(ASCO-VF)、欧洲肿瘤内科学会-临床获益幅度量表(ESMO-MCBS)和法国 HTA 标准,即临床附加价值(CAV)评估其 ATB。后者的评分决定了报销和国家市场准入。39 项适应证中的 35 种药物获得了 ATU。所有药物均获得上市许可,并具有临床获益,可由社会保险报销。与现有疗法相比,28 种(71.8%)药物具有 CAV。24/38(63.2%)种药物的 ESMO-MCBS 评分在 4-5 分之间,19/33(57.6%)种药物的 ASCO-VF 评分在 45 分以上。未发现成本、PFS、OS、CAV 和 ASCO-VF 评分之间存在相关性,而 ESMO-MCBS 评分较高与 OS 相关。总之,许多患者在获得上市许可之前就通过 ATU 接受了创新药物治疗,尽管 ATB 评分之间存在差异,因此评估创新疗法时国际合作非常重要。