Infectious Diseases Division, icddrb, Dhaka, Bangladesh.
Health Systems and Population Studies Division, icddrb, Dhaka, Bangladesh.
PLoS One. 2022 May 23;17(5):e0268093. doi: 10.1371/journal.pone.0268093. eCollection 2022.
Seroprevalence studies have been carried out in many developed and developing countries to evaluate ongoing and past infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Data on this infection in marginalized populations in urban slums are limited, which may offer crucial information to update prevention and mitigation policies and strategies. We aimed to determine the seroprevalence of SARS-CoV-2 infection and factors associated with seropositivity in slum and non-slum communities in two large cities in Bangladesh.
A cross-sectional study was carried out among the target population in Dhaka and Chattogram cities between October 2020 and February 2021. Questionnaire-based data, anthropometric and blood pressure measurements and blood were obtained. SARS-CoV-2 serology was assessed by Roche Elecsys® Anti-SARS-CoV-2 immunoassay.
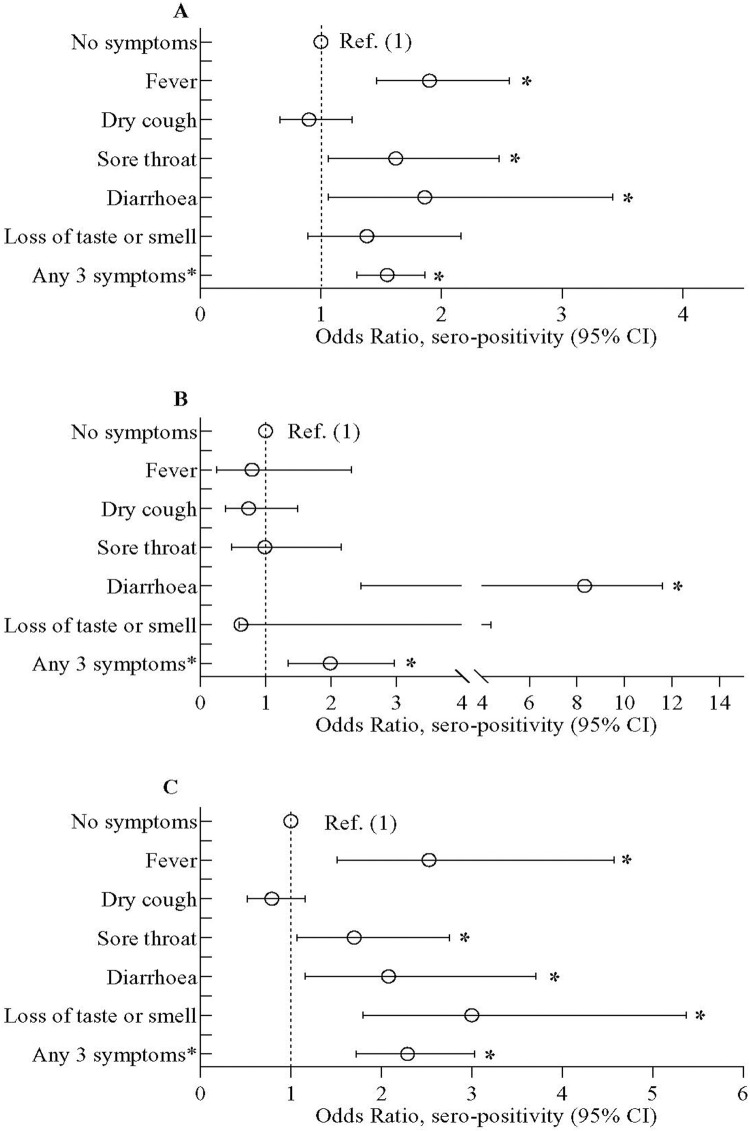
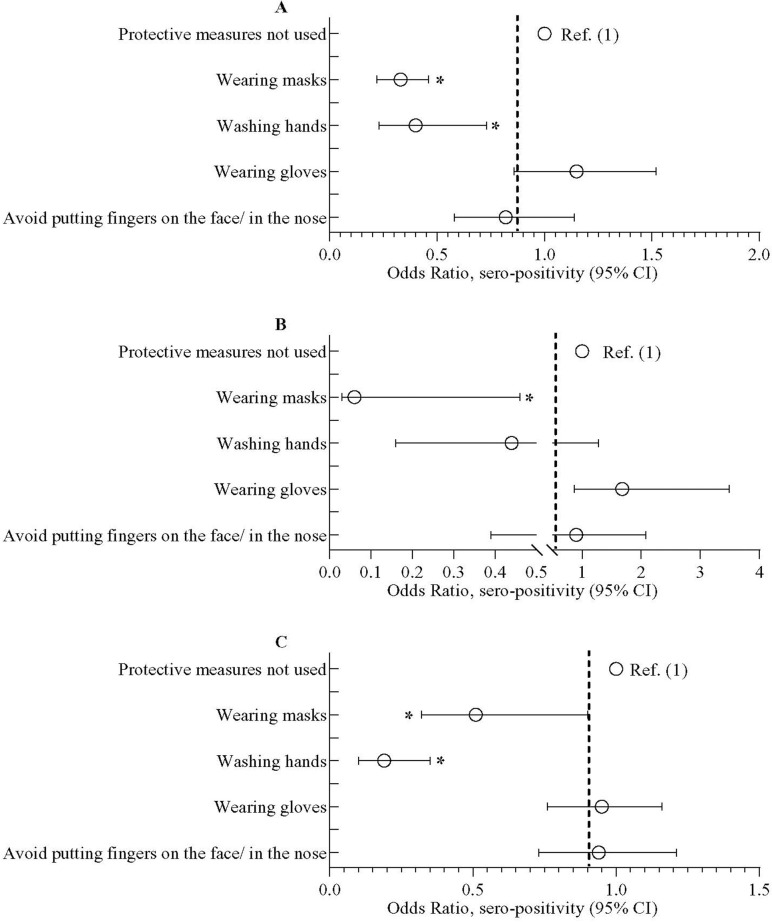
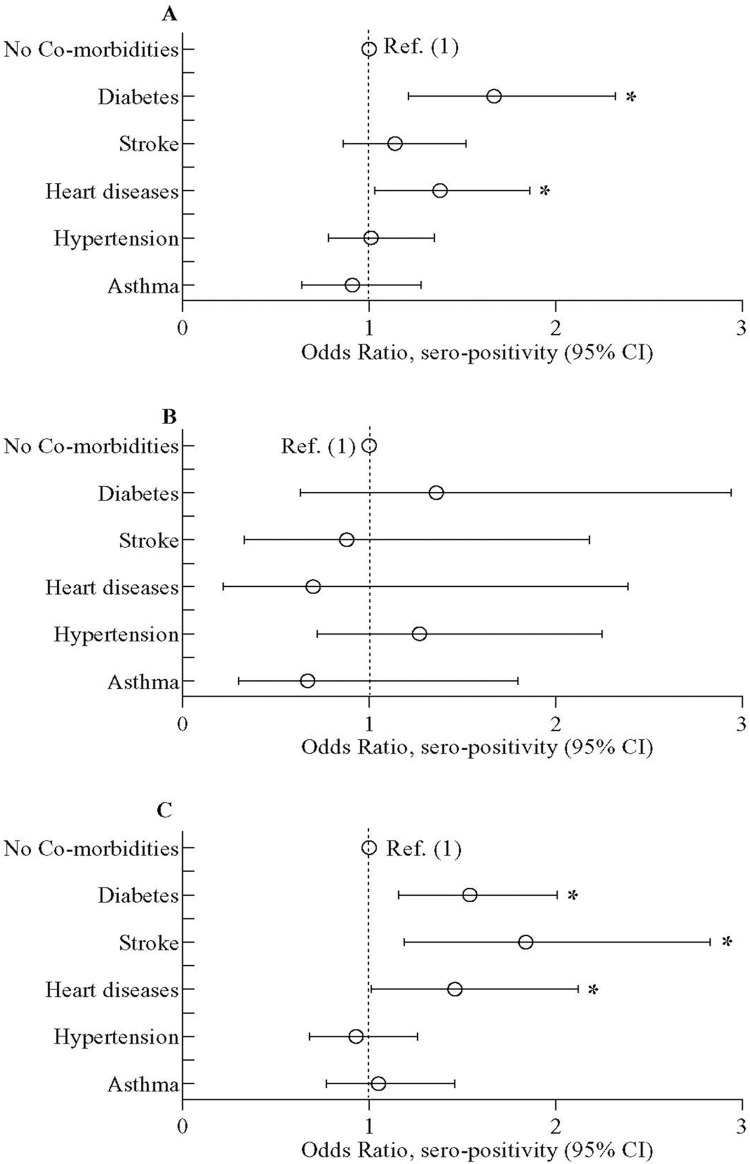
Among the 3220 participants (2444 adults, ≥18 years; 776 children, 10-17 years), the overall weighted seroprevalence was 67.3% (95% confidence intervals (CI) = 65.2, 69.3) with 71.0% in slum (95% CI = 68.7, 72.2) and 62.2% in non-slum (95% CI = 58.5, 65.8). The weighted seroprevalence was 72.9% in Dhaka and 54.2% in Chattogram. Seroprevalence was positively associated with limited years of formal education (adjusted odds ratio [aOR] = 1.61; 95% CI = 1.43, 1.82), lower income (aOR = 1.23; 95% CI = 1.03, 1.46), overweight (aOR = 1.2835; 95% CI = 1.26, 1.97), diabetes (aOR = 1.67; 95% CI = 1.21, 2.32) and heart disease (aOR = 1.38; 95% CI = 1.03, 1.86). Contrarily, negative associations were found between seropositivity and regular wearing of masks and washing hands, and prior BCG vaccination. About 63% of the population had asymptomatic infection; only 33% slum and 49% non-slum population showed symptomatic infection.
The estimated seroprevalence of SARS-CoV-2 was more prominent in impoverished informal settlements than in the adjacent middle-income non-slum areas. Additional factors associated with seropositivity included limited education, low income, overweight and pre-existing chronic conditions. Behavioral factors such as regular wearing of masks and washing hands were associated with lower probability of seropositivity.
许多发达国家和发展中国家都开展了血清流行率研究,以评估严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)的持续和既往感染情况。城市贫民窟中边缘化人群的感染数据有限,这可能为更新预防和缓解政策和策略提供关键信息。我们旨在确定孟加拉国两个大城市的贫民窟和非贫民窟社区中 SARS-CoV-2 感染的血清流行率以及与血清阳性相关的因素。
2020 年 10 月至 2021 年 2 月期间,在达卡和吉大港市的目标人群中进行了横断面研究。收集了基于问卷的资料、人体测量和血压测量以及血液样本。使用罗氏 Elecsys® Anti-SARS-CoV-2 免疫分析试剂盒评估 SARS-CoV-2 血清学。
在 3220 名参与者(2444 名成年人,≥18 岁;776 名儿童,10-17 岁)中,总体加权血清流行率为 67.3%(95%置信区间[CI] = 65.2,69.3),贫民窟为 71.0%(95% CI = 68.7,72.2),非贫民窟为 62.2%(95% CI = 58.5,65.8)。达卡的加权血清流行率为 72.9%,而吉大港为 54.2%。血清流行率与正规教育年限有限(调整优势比[aOR] = 1.61;95% CI = 1.43,1.82)、收入较低(aOR = 1.23;95% CI = 1.03,1.46)、超重(aOR = 1.2835;95% CI = 1.26,1.97)、糖尿病(aOR = 1.67;95% CI = 1.21,2.32)和心脏病(aOR = 1.38;95% CI = 1.03,1.86)呈正相关。相反,血清阳性与经常戴口罩和洗手以及先前的卡介苗接种呈负相关。约 63%的人口存在无症状感染;只有 33%的贫民窟和 49%的非贫民窟人口出现症状性感染。
在贫困的非正规住区中,估计的 SARS-CoV-2 血清流行率比相邻的中等收入非贫民窟地区更为突出。与血清阳性相关的其他因素包括受教育程度有限、收入低、超重和先前存在的慢性疾病。经常戴口罩和洗手等行为因素与较低的血清阳性概率相关。