Van Dessel Eleni D, De Meyer Gregory R, Morrison Stuart G, Jorens Philippe G, Schepens Tom
Department of Critical Care Medicine, Antwerp University Hospital/University of Antwerp, Drie Eikenstraat 655, 2650, Edegem, Belgium.
Department of Anesthesiology, Antwerp University Hospital/University of Antwerp, Edegem, Belgium.
Intensive Care Med Exp. 2022 May 24;10(1):19. doi: 10.1186/s40635-022-00449-4.
Flow-controlled ventilation (FCV), a novel mode of mechanical ventilation characterised by constant flow during active expiration, may result in more efficient alveolar gas exchange, better lung recruitment and might be useful in limiting ventilator-induced lung injury. However, data regarding FCV in mechanically ventilated patients with acute lung injury or acute respiratory distress syndrome (ARDS) are scarce.
We hypothesised that the use of FCV is feasible and would improve oxygenation in moderate COVID-19 ARDS compared to conventional ventilation.
Open-label repeated-measures controlled trial.
From February to April 2021, patients with moderate COVID-19 ARDS were recruited in a tertiary referral intensive care unit.
Patients with moderate ARDS (PO/FO ratio 100-200 mmHg, SpO 88-94% and PO 60-80 mmHg) were considered eligible. Exclusion criteria were: extremes of age (< 18 years, > 80 years), obesity (body mass index > 40 kg/m), prone positioning at the time of intervention, mechanical ventilation for more than 10 days and extracorporeal membrane oxygenation. Eleven patients were recruited.
Participants were ventilated in FCV mode for 30 min, and subsequently in volume-control mode (VCV) for 30 min.
Feasibility of FCV to maintain oxygenation was assessed by the PO/FO ratio (mmHg) as a primary outcome parameter. Secondary outcomes included ventilator parameters, PCO and haemodynamic data. All adverse events were recorded.
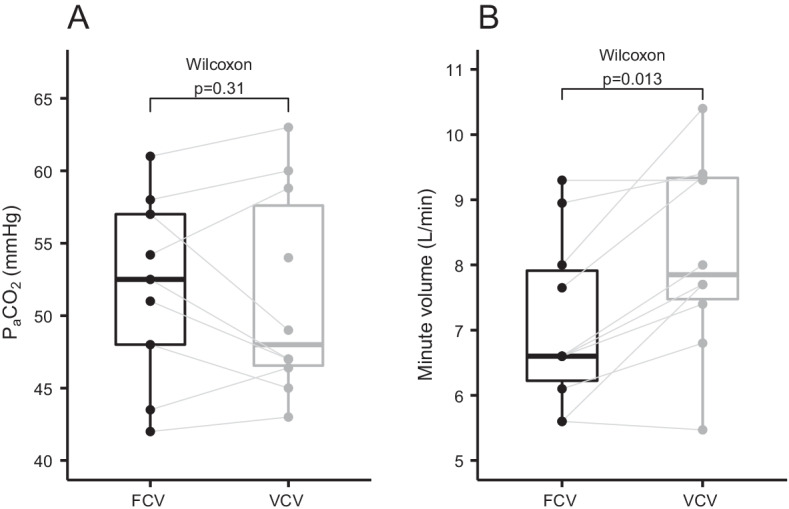
FCV was feasible in all patients and no adverse events were observed. There was no difference in the PaO2/FIO2 ratio after 30 min of ventilation in FCV mode (169 mmHg) compared to 30 min of ventilation in VCV mode subsequently (168 mmHg, 95% CI of pseudo-medians (- 10.5, 3.6), p = 0.56). The tidal volumes (p < 0.01) and minute ventilation were lower during FCV (p = 0.01) while PaCO2 was similar at the end of the 30-min ventilation periods (p = 0.31). Mean arterial pressure during FCV was comparable to baseline.
Thirty minutes of FCV in patients with moderate COVID-19 ARDS receiving neuromuscular blocking agents resulted in similar oxygenation, compared to VCV. FCV was feasible and did not result in adverse events.
Clinicaltrials.gov identifier: NCT04894214.
流量控制通气(FCV)是一种新型机械通气模式,其特点是在主动呼气过程中流量恒定,可能会使肺泡气体交换更高效,更好地实现肺复张,并且可能有助于限制呼吸机诱发的肺损伤。然而,关于急性肺损伤或急性呼吸窘迫综合征(ARDS)机械通气患者使用FCV的数据很少。
我们假设,与传统通气相比,在中度新型冠状病毒肺炎(COVID-19)ARDS患者中使用FCV是可行的,并且能改善氧合。
开放标签重复测量对照试验。
2021年2月至4月,在一家三级转诊重症监护病房招募中度COVID-19 ARDS患者。
中度ARDS患者(氧合指数100 - 200 mmHg,脉搏血氧饱和度88 - 94%,动脉血氧分压60 - 80 mmHg)被认为符合条件。排除标准为:年龄极端情况(<18岁,>80岁)、肥胖(体重指数>40 kg/m²)、干预时俯卧位、机械通气超过10天以及体外膜肺氧合。招募了11名患者。
参与者先以FCV模式通气30分钟,随后以容量控制模式(VCV)通气30分钟。
以氧合指数(mmHg)作为主要结局参数评估FCV维持氧合的可行性。次要结局包括呼吸机参数、二氧化碳分压和血流动力学数据。记录所有不良事件。
FCV在所有患者中均可行,未观察到不良事件。与随后30分钟的VCV模式通气(168 mmHg,伪中位数的95%置信区间为(-10.5, 3.6),p = 0.56)相比,FCV模式通气30分钟后的动脉血氧分压/吸入氧分数值无差异(169 mmHg)。FCV期间潮气量(p < 0.01)和分钟通气量较低(p = 0.01),而在30分钟通气期结束时二氧化碳分压相似(p = 0.31)。FCV期间平均动脉压与基线相当。
对于接受神经肌肉阻滞剂治疗的中度COVID-19 ARDS患者,30分钟的FCV与VCV相比,氧合效果相似。FCV是可行的,且未导致不良事件。
Clinicaltrials.gov标识符:NCT04894214。