Lancet Glob Health. 2022 Jul;10(7):e1003-e1011. doi: 10.1016/S2214-109X(22)00168-1. Epub 2022 May 24.
Early death after cancer surgery is higher in low-income and middle-income countries (LMICs) compared with in high-income countries, yet the impact of facility characteristics on early postoperative outcomes is unknown. The aim of this study was to examine the association between hospital infrastructure, resource availability, and processes on early outcomes after cancer surgery worldwide.
A multimethods analysis was performed as part of the GlobalSurg 3 study-a multicentre, international, prospective cohort study of patients who had surgery for breast, colorectal, or gastric cancer. The primary outcomes were 30-day mortality and 30-day major complication rates. Potentially beneficial hospital facilities were identified by variable selection to select those associated with 30-day mortality. Adjusted outcomes were determined using generalised estimating equations to account for patient characteristics and country-income group, with population stratification by hospital.
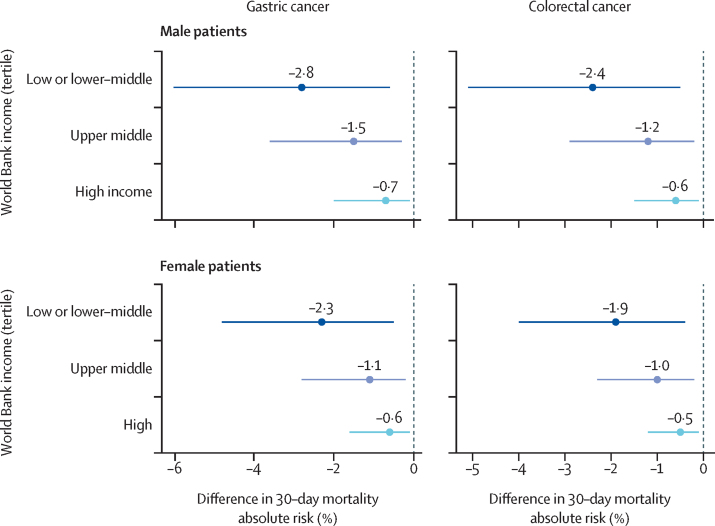
Between April 1, 2018, and April 23, 2019, facility-level data were collected for 9685 patients across 238 hospitals in 66 countries (91 hospitals in 20 high-income countries; 57 hospitals in 19 upper-middle-income countries; and 90 hospitals in 27 low-income to lower-middle-income countries). The availability of five hospital facilities was inversely associated with mortality: ultrasound, CT scanner, critical care unit, opioid analgesia, and oncologist. After adjustment for case-mix and country income group, hospitals with three or fewer of these facilities (62 hospitals, 1294 patients) had higher mortality compared with those with four or five (adjusted odds ratio [OR] 3·85 [95% CI 2·58-5·75]; p<0·0001), with excess mortality predominantly explained by a limited capacity to rescue following the development of major complications (63·0% vs 82·7%; OR 0·35 [0·23-0·53]; p<0·0001). Across LMICs, improvements in hospital facilities would prevent one to three deaths for every 100 patients undergoing surgery for cancer.
Hospitals with higher levels of infrastructure and resources have better outcomes after cancer surgery, independent of country income. Without urgent strengthening of hospital infrastructure and resources, the reductions in cancer-associated mortality associated with improved access will not be realised.
National Institute for Health and Care Research.
与高收入国家相比,癌症手术后的早期死亡率在中低收入国家(LMICs)更高,但是医疗机构的特点对术后早期结果的影响尚不清楚。本研究旨在检查全球范围内癌症手术后医院基础设施、资源可用性和流程与早期结果之间的关联。
作为全球 Surg 3 研究的一部分,采用多方法分析-对接受乳腺癌、结直肠癌或胃癌手术的患者进行的多中心、国际、前瞻性队列研究。主要结果是 30 天死亡率和 30 天主要并发症发生率。通过变量选择确定潜在有益的医院设施,以选择与 30 天死亡率相关的设施。使用广义估计方程确定调整后的结果,以考虑患者特征和国家收入组,并按医院进行人群分层。
在 2018 年 4 月 1 日至 2019 年 4 月 23 日期间,在 66 个国家的 238 家医院共收集了 9685 名患者的设施水平数据(20 个高收入国家的 91 家医院;19 个中高收入国家的 57 家医院;27 个低收入和中低收入国家的 90 家医院)。五种医院设施的可用性与死亡率呈负相关:超声、CT 扫描仪、重症监护病房、阿片类镇痛药和肿瘤医生。在调整病例组合和国家收入组后,与拥有四到五种这些设施的医院(调整后的优势比[OR]3.85[95%CI 2.58-5.75];p<0.0001)相比,拥有三种或更少这些设施的医院(62 家医院,1294 名患者)的死亡率更高,这主要是由于在发生重大并发症后挽救能力有限(63.0%对 82.7%;OR 0.35[0.23-0.53];p<0.0001)。在整个中低收入国家,改善医院设施可预防每 100 名接受癌症手术的患者中出现 1 至 3 例死亡。
基础设施和资源水平较高的医院在癌症手术后的结果更好,而与国家收入无关。如果不紧急加强医院基础设施和资源,那么改善获得治疗的机会所带来的与癌症相关的死亡率降低将无法实现。
国家卫生与保健研究中心。