ElmediX NV, 2800 Mechelen, Belgium.
Laboratory of Cell Biology and Histology, Faculty of Medicine and Health Sciences, University of Antwerp, 2610 Antwerp, Belgium.
Biomolecules. 2022 Apr 29;12(5):651. doi: 10.3390/biom12050651.
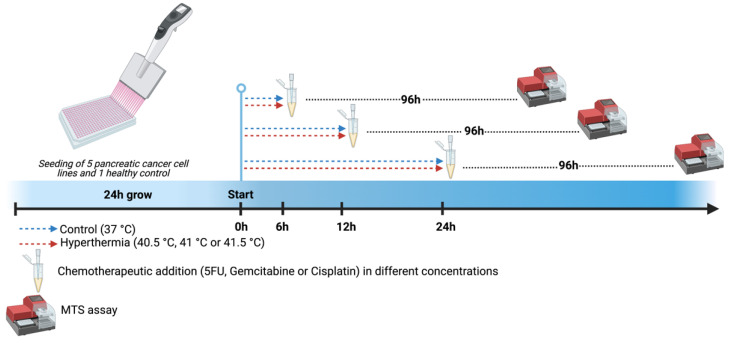
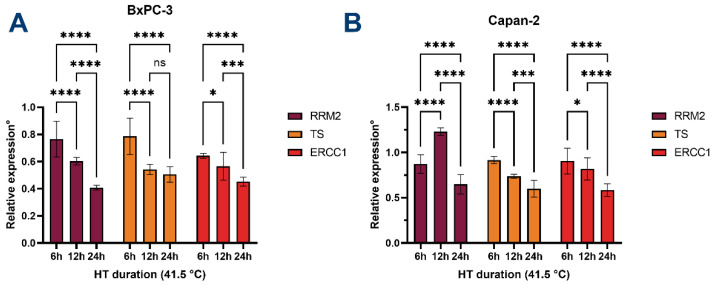
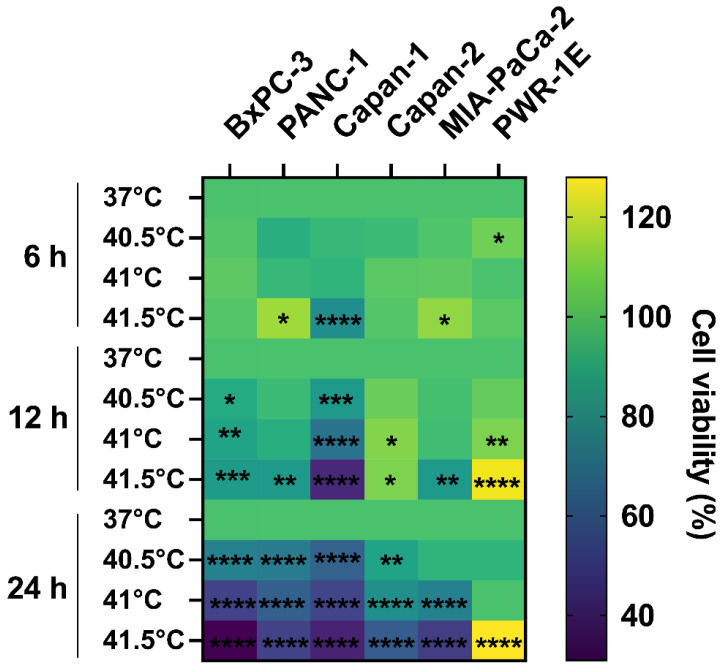
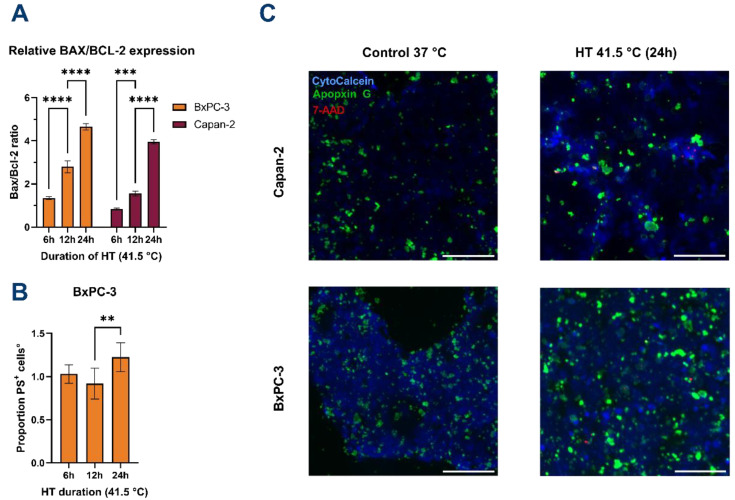
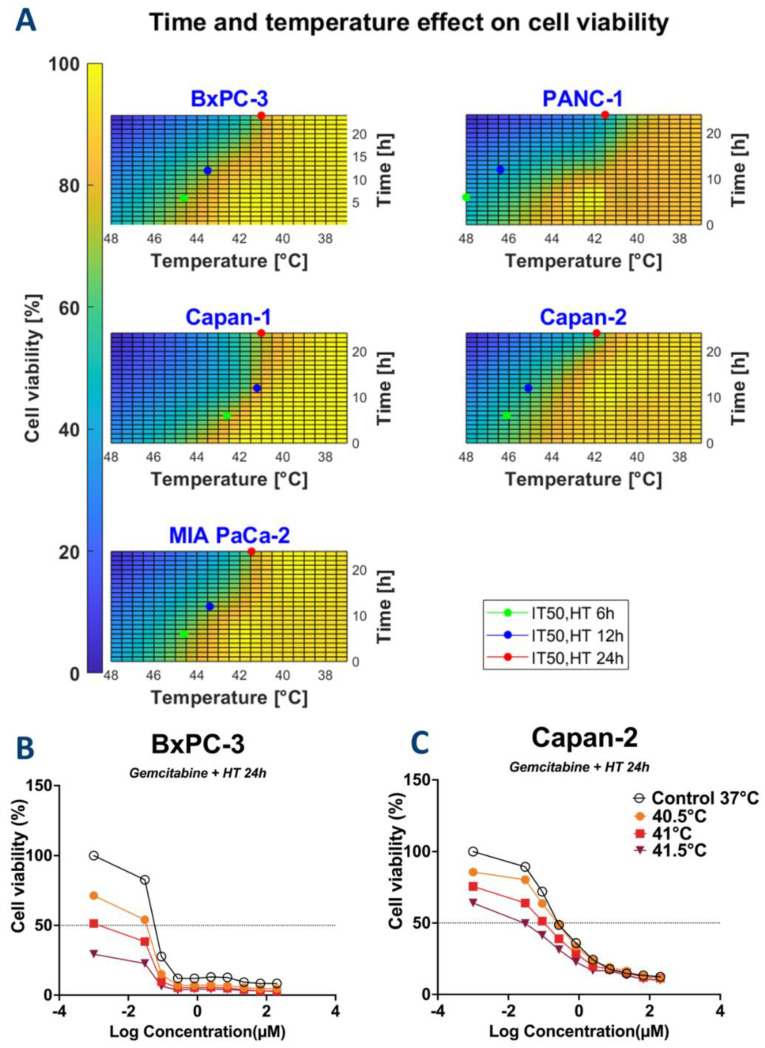
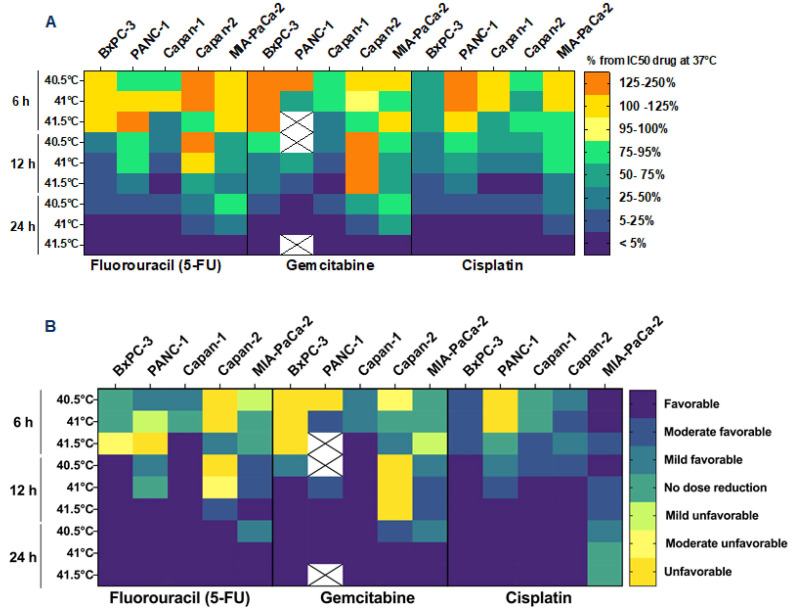
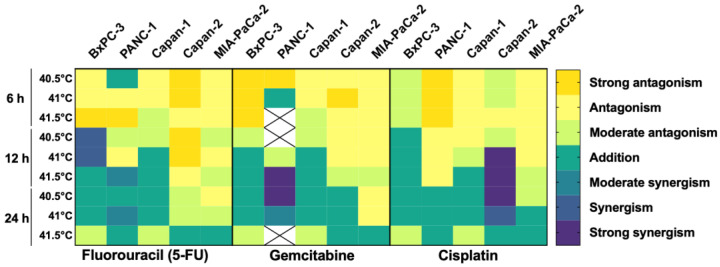
Chemotherapy (CT) is the standard care for advanced pancreatic ductal adenocarcinoma (PDAC); however, with limited efficacy. Hyperthermia (HT) treatment has been suggested as a sensitizer to improve outcomes. However, the direct effect of the HT and CT combination is not fully understood. Therefore, we aim to assess the direct cytotoxic effect of HT in PDAC cells as monotherapy or in combination with chemotherapeutics. Different temperatures (37-, 40.5-, 41-, and 41.5 °C) and durations (6-, 12-, and 24 h) were tested in PDAC cell lines (BxPC-3, Capan-1, Capan-2, PANC-1, and MIA-PaCa-2). Different concentrations of gemcitabine, 5-fluorouracil, and cisplatin were also tested in these conditions. The impact on cell metabolic activity was determined by an MTS assay. Enhancement of chemosensitivity was assessed by a reduction in half-maximal inhibitory concentration (IC50). HT and chemotherapeutics interactions were classified as antagonistic, additive, or synergistic using the combination index. HT inhibited cell proliferation in a cell type, temperature, and duration-dependent manner. The induction of apoptosis was seen after 6 h of HT treatment, eventually followed by secondary necrosis. The HT and CT combination led to an IC50 reduction of the tested CT. At 12 h of HT, this effect was between 25 to 90% and reached a 95% reduction at 24 h. The additive or synergistic effect was demonstrated in all cell lines and chemotherapeutics, although, again, this depended on cell type, duration, and temperature. HT is cytotoxic and enhances the therapeutic effectiveness of gemcitabine, 5-fluorouracil, and cisplatin on PDAC cells. This result was further confirmed by the decrease in the expression of , , and in BxPC-3 and Capan-2 cells. These observations warrant further study in specific subsets of PDAC patients to improve their clinical outcomes.
化疗(CT)是晚期胰腺导管腺癌(PDAC)的标准治疗方法;然而,疗效有限。热疗(HT)治疗已被提议作为一种增敏剂来改善结果。然而,HT 和 CT 联合的直接作用尚未完全理解。因此,我们旨在评估 HT 作为单一疗法或与化疗联合治疗 PDAC 细胞的直接细胞毒性作用。在 PDAC 细胞系(BxPC-3、Capan-1、Capan-2、PANC-1 和 MIA-PaCa-2)中测试了不同的温度(37、40.5、41 和 41.5°C)和持续时间(6、12 和 24 h)。在这些条件下还测试了不同浓度的吉西他滨、5-氟尿嘧啶和顺铂。通过 MTS 测定法确定对细胞代谢活性的影响。通过降低半最大抑制浓度(IC50)来评估化疗敏感性的增强。使用组合指数将 HT 和化疗药物的相互作用分类为拮抗、相加或协同。HT 以细胞类型、温度和持续时间依赖的方式抑制细胞增殖。在 HT 治疗 6 小时后观察到细胞凋亡的诱导,最终继发坏死。HT 和 CT 联合导致测试 CT 的 IC50 降低。在 HT 12 小时时,这种作用在 25%到 90%之间,在 24 小时时达到 95%的降低。在所有细胞系和化疗药物中均显示出相加或协同作用,尽管这种作用再次取决于细胞类型、持续时间和温度。HT 具有细胞毒性作用,并增强了吉西他滨、5-氟尿嘧啶和顺铂对 PDAC 细胞的治疗效果。这一结果在 BxPC-3 和 Capan-2 细胞中 、 和 的表达减少中得到进一步证实。这些观察结果证明在特定的 PDAC 患者亚群中进一步研究以改善其临床结果是合理的。