Belloni Elena, Muttillo Edoardo Maria, Di Saverio Salomone, Gasparrini Marcello, Brescia Antonio, Nigri Giuseppe
Oncologic Colorectal Surgical Unit and Robotic Surgery Unit, Department of Medical and Surgical Sciences and Translational Medicine, Sapienza University of Rome, 00189 Rome, Italy.
Department of General Surgery, ASUR Marche, AV5, Hospital of San Benedetto del Tronto, 63074 San Benedetto del Tronto, Italy.
Cancers (Basel). 2022 May 13;14(10):2411. doi: 10.3390/cancers14102411.
In rectal cancer surgery, anastomotic leakage (AL) remains the most feared complication, with a frequency of up to 30% in non-high-volume centers. The preservation of proper vascularization is a key factor for successful anastomosis. The use of fluorescence with indocyanine green (ICG) as an intraoperative method to verify optimal perfusion is becoming an interesting tool in rectal surgery. Today, robotic surgery, together with the use of the intraoperative evaluation of the perfusion with ICG, could be a real strategy to deal with AL, allowing for a more delicate and less traumatic surgical technique. This strategy may allow for an extremely accurate surgery, and for optimal control of the proper vascularization of the rectum.
The purpose of this descriptive review is to analyze the impact of fluorescence and robotic surgery on short-term surgical outcomes for rectal cancer.
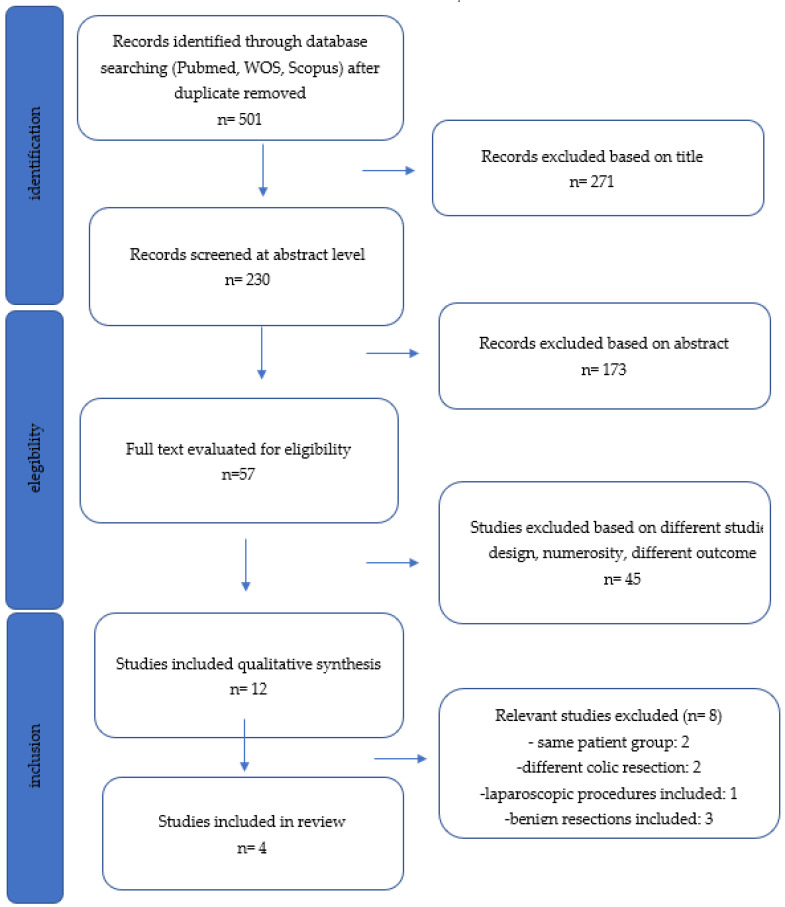
We performed a systematic literature search using the PubMed, Embase and Cochrane library databases. The primary endpoints were to evaluate the application of ICG fluorescence in robotic rectal surgery and the rate of anastomotic leakage when using these technological implementations. The secondary endpoints were to evaluate the dosage of ICG and the timing of application by different surgeons.
ICG fluorescence is an inexpensive and quick method to assess bowel perfusion, providing immediate feedback to the surgeon, even if its role has not been proven. A quantitative system must be systematically introduced to minimize the subjectiveness of the visualized image.
在直肠癌手术中,吻合口漏(AL)仍然是最令人担忧的并发症,在非高容量中心其发生率高达30%。保留适当的血管化是吻合成功的关键因素。使用吲哚菁绿(ICG)荧光作为术中验证最佳灌注的方法,正成为直肠癌手术中一种有趣的工具。如今,机器人手术以及术中使用ICG评估灌注情况,可能是应对吻合口漏的一种切实可行的策略,能实现更精细、创伤更小的手术技术。这种策略可能使手术极其精确,并能对直肠的适当血管化进行最佳控制。
本描述性综述的目的是分析荧光和机器人手术对直肠癌短期手术结果的影响。
我们使用PubMed、Embase和Cochrane图书馆数据库进行了系统的文献检索。主要终点是评估ICG荧光在机器人直肠癌手术中的应用以及使用这些技术手段时的吻合口漏发生率。次要终点是评估不同外科医生使用ICG的剂量和应用时机。
ICG荧光是一种评估肠管灌注的廉价且快速的方法,能为外科医生提供即时反馈,尽管其作用尚未得到证实。必须系统地引入定量系统,以尽量减少可视化图像的主观性。