Department of General, Visceral, Transplant, Vascular and Pediatric Surgery at Würzburg University Hospital, Würzburg, Germany.
Department of Visceral, Transplant, Thoracic and Vascular Surgery at Leipzig University Hospital, Leipzig, Germany.
Langenbecks Arch Surg. 2022 Sep;407(6):2481-2488. doi: 10.1007/s00423-022-02568-8. Epub 2022 May 28.
In selected cases of severe Cushing's syndrome due to uncontrolled ACTH secretion, bilateral adrenalectomy appears unavoidable. Compared with unilateral adrenalectomy (for adrenal Cushing's syndrome), bilateral adrenalectomy has a perceived higher perioperative morbidity. The aim of the current study was to compare both interventions in endogenous Cushing's syndrome regarding postoperative outcomes.
We report a single-center, retrospective cohort study comparing patients with hypercortisolism undergoing bilateral vs. unilateral adrenalectomy during 2008-2021. Patients with adrenal Cushing's syndrome due to adenoma were compared with patients with ACTH-dependent Cushing's syndrome (Cushing's disease and ectopic ACTH production) focusing on postoperative morbidity and mortality as well as long-term survival.
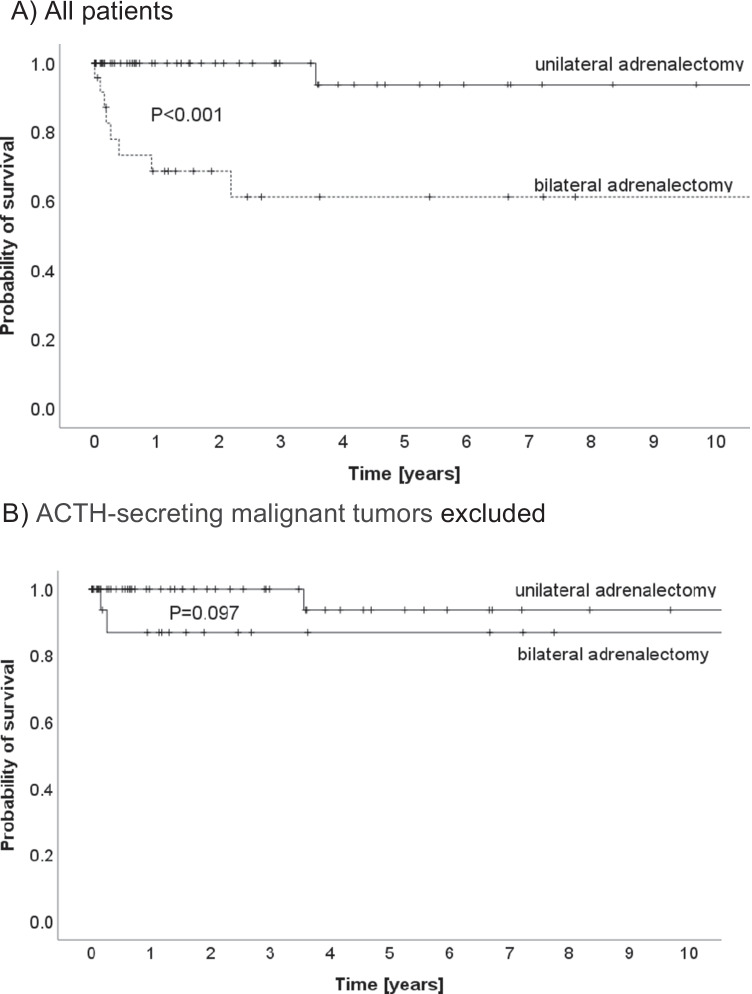
Of 83 patients with adrenalectomy for hypercortisolism (65.1% female, median age 53 years), the indication for adrenalectomy was due to adrenal Cushing's syndrome in 60 patients (72.2%; 59 unilateral and one bilateral), and due to hypercortisolism caused by Cushing's disease (n = 16) or non-pituitary uncontrolled ACTH secretion of unknown origin (n = 7) (27.7% of all adrenalectomies). Compared with unilateral adrenalectomy (n = 59), patients with bilateral adrenalectomy (n = 24) had a higher rate of severe complications (0% vs. 33%; p < 0.001) and delayed recovery (median: 10.2% vs. 79.2%; p < 0.001). Using the MTL30 marker, patients with bilateral adrenalectomy fared worse than patients after unilateral surgery (MTL30 positive: 7.2% vs. 25.0% p < 0.001). Postoperative mortality was increased in patients with bilateral adrenalectomy (0% vs. 8.3%; p = 0.081).
While unilateral adrenalectomy for adrenal Cushing's syndrome represents a safe and definitive therapeutic option, bilateral adrenalectomy to control ACTH-dependent extra-adrenal Cushing's syndrome or Cushing's disease is a more complicated intervention with a mortality of nearly 10%.
在某些因 ACTH 分泌失控导致的严重库欣综合征病例中,双侧肾上腺切除术似乎是不可避免的。与单侧肾上腺切除术(用于肾上腺库欣综合征)相比,双侧肾上腺切除术的围手术期发病率更高。本研究的目的是比较内源性库欣综合征中这两种干预措施的术后结果。
我们报告了一项单中心回顾性队列研究,比较了 2008 年至 2021 年间因库欣综合征接受双侧或单侧肾上腺切除术的患者。比较了因腺瘤导致肾上腺库欣综合征的患者与因 ACTH 依赖性库欣综合征(库欣病和异位 ACTH 分泌)导致的患者,重点关注术后发病率和死亡率以及长期生存率。
在 83 例因库欣综合征行肾上腺切除术的患者中(65.1%为女性,中位年龄 53 岁),肾上腺切除术的指征为肾上腺库欣综合征 60 例(72.2%;59 例单侧,1 例双侧),库欣病(n=16)或非垂体不明原因的不受控制的 ACTH 分泌(n=7)导致的库欣综合征(所有肾上腺切除术的 27.7%)。与单侧肾上腺切除术(n=59)相比,双侧肾上腺切除术(n=24)患者的严重并发症发生率更高(0% vs. 33%;p<0.001),恢复时间延迟(中位数:10.2% vs. 79.2%;p<0.001)。使用 MTL30 标志物,双侧肾上腺切除术患者的预后不如单侧手术患者(MTL30 阳性:7.2% vs. 25.0%;p<0.001)。双侧肾上腺切除术患者的术后死亡率增加(0% vs. 8.3%;p=0.081)。
单侧肾上腺切除术治疗肾上腺库欣综合征是一种安全且明确的治疗选择,而双侧肾上腺切除术用于控制 ACTH 依赖性肾上腺外库欣综合征或库欣病则是一种更复杂的干预措施,死亡率接近 10%。