Department of Anesthesia, Intensive Care and Prehospital Emergency Service, Maggiore Hospital Carlo Alberto Pizzardi, Bologna, Italy.
Department of Anesthesia and Intensive Care Medicine, IRCCS Humanitas Research Hospital, Rozzano, Milano, Italy
BMJ Open. 2022 May 30;12(5):e062097. doi: 10.1136/bmjopen-2022-062097.
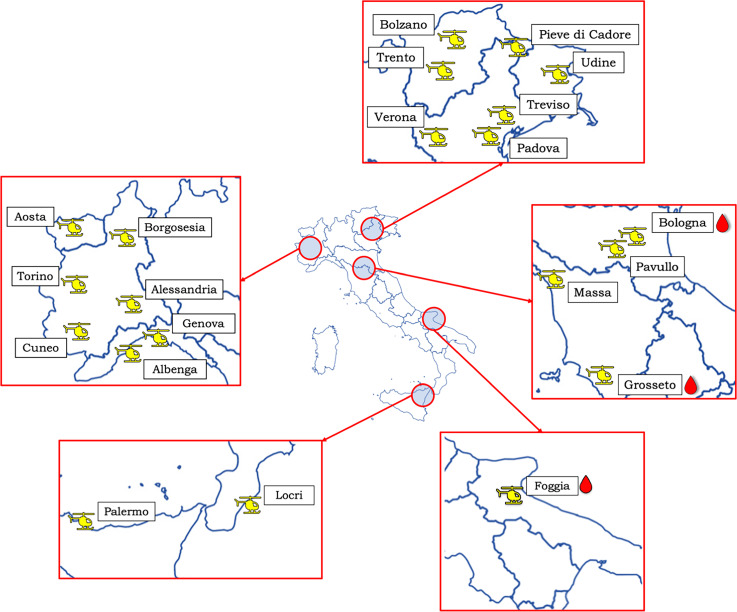
Major haemorrhage after injury is the leading cause of preventable death for trauma patients. Recent advancements in trauma care suggest damage control resuscitation (DCR) should start in the prehospital phase following major trauma. In Italy, Helicopter Emergency Medical Services (HEMS) assist the most complex injuries and deliver the most advanced interventions including DCR. The effect size of DCR delivered prehospitally on survival remains however unclear.
This is an investigator-initiated, large, national, prospective, observational cohort study aiming to recruit >500 patients in haemorrhagic shock after major trauma. We aim at describing the current practice of hypotensive trauma management as well as propose the creation of a national registry of patients with haemorrhagic shock.
the exploration of the effect size of the variation in clinical practice on the mortality of hypotensive trauma patients. The primary outcome measure will be 24 hours, 7-day and 30-day mortality. Secondary outcomes include: association of prehospital factors and survival from injury to hospital admission, hospital length of stay, prehospital and in-hospital complications, hospital outcomes; use of prehospital ultrasound; association of prehospital factors and volume of first 24-hours blood product administration and evaluation of the prevalence of use, appropriateness, haemodynamic, metabolic and effects on mortality of prehospital blood transfusions.
age >18 years, traumatic injury attended by a HEMS team including a physician, a systolic blood pressure <90 mm Hg or weak/absent radial pulse and a confirmed or clinically likely diagnosis of major haemorrhage. Prehospital and in-hospital variables will be collected to include key times, clinical findings, examinations and interventions. Patients will be followed-up until day 30 from admission. The Glasgow Outcome Scale Extended will be collected at 30 days from admission.
The study has been approved by the Ethics committee 'Comitato Etico di Area Vasta Emilia Centro'. Data will be disseminated to the scientific community by abstracts submitted to international conferences and by original articles submitted to peer-reviewed journals.
NCT04760977.
创伤后大出血是创伤患者可预防死亡的主要原因。最近创伤救治的进展表明,损伤控制性复苏(DCR)应在重大创伤后开始进行院前阶段。在意大利,直升机紧急医疗服务(HEMS)协助处理最复杂的损伤,并提供包括 DCR 在内的最先进的干预措施。然而,院前实施 DCR 对生存率的影响大小仍不清楚。
这是一项由调查员发起的、大型的、全国性的、前瞻性的、观察性队列研究,旨在招募 500 多名创伤后失血性休克患者。我们旨在描述目前的低血压创伤管理实践,并提出建立一个失血性休克患者的全国登记处。
探索临床实践变异对低血压创伤患者死亡率的影响大小。主要结局测量指标为 24 小时、7 天和 30 天死亡率。次要结局包括:院前因素与从受伤到入院期间的生存率、住院时间、院前和院内并发症、医院结局的关联;院前超声的使用;院前因素与前 24 小时血液制品给药量的关联,以及评估院前输血的使用频率、适当性、血流动力学、代谢和对死亡率的影响。
年龄>18 岁,由 HEMS 团队处理的创伤性损伤,包括一名医生,收缩压<90mmHg 或桡动脉脉搏微弱/消失,以及明确或临床可能的大出血诊断。将收集院前和院内变量,包括关键时间、临床发现、检查和干预。将对患者进行随访,直到入院后 30 天。入院后 30 天将收集格拉斯哥预后扩展量表。
该研究已获得伦理委员会'Comitato Etico di Area Vasta Emilia Centro'的批准。将通过向国际会议提交摘要和向同行评议期刊提交原始文章,向科学界传播数据。
NCT04760977。