Zini Radaelli Lorenzo Federico, Aramini Beatrice, Ciarrocchi Angelo Paolo, Sanna Stefano, Argnani Desideria, Stella Franco
Division of Thoracic Surgery, Department of Experimental, Diagnostic and Specialty Medicine - DIMES Alma Mater Studiorum - University of Bologna, G.B. Morgagni-L. Pierantoni Hospital, Via Carlo Forlanini 34, Forlì, Italy.
Ann Med Surg (Lond). 2022 Apr 14;77:103630. doi: 10.1016/j.amsu.2022.103630. eCollection 2022 May.
Achalasia with megaesophagus is a pathology characterized by widespread and irregular dilation of the esophageal lumen. In most cases, this dilation is caused by contraction and subsequent failed relaxation of the lower esophageal sphincter (LES). It may be associated with a partial or complete slowing of the esophageal peristalsis.
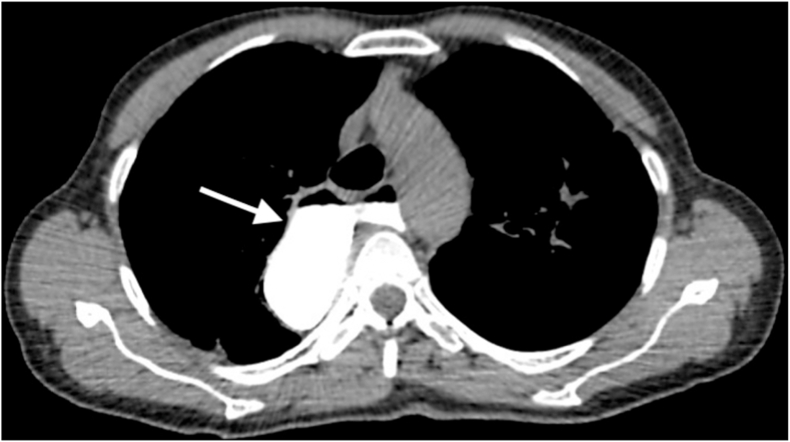
We present the case of a 58-year-old woman who developed dysphagia, regurgitation, and substantial weight loss (11 kg) over a span of 1 year. Symptomatic achalasia with megaesophagus was diagnosed following chest and abdominal computed tomography (CT) with contrast and transit RX with gastrografin and esophageal manometry. The patient refuse all minimally endoscopic treatments and opted straightly for the treatment with esophagectomy sec. Ivor-Lewis. At the 6-month follow-up, the patient appeared in excellent general clinical condition and oral gastrografin radiography (OGR) showed good channeling.
Patients require medical attention when presenting with achalasia that has eroded the esophageal wall enough to form a megaesophagus. Early and minimally invasive treatments (i.e., medical therapy, endoscopic dilation, and myotomy) are insufficient at this stage, and thus esophageal surgery is required. Among the most common surgical approaches, we must mention esophagectomy sec. McKeown and esophagectomy with interposition of a colic loop sec. Wilkins; however, based on our experience, esophagectomy sec. Ivor-Lewis with intrathoracic anastomosis leads to excellent results and can therefore be considered a valid alternative for treating complex cases.
Subtotal esophagectomy sec. Ivor-Lewis with intrathoracic anastomosis is effective in treating achalasia with megaesophagus.
贲门失弛缓症合并巨食管是一种以食管腔广泛且不规则扩张为特征的病理状态。在大多数情况下,这种扩张是由食管下括约肌(LES)收缩及随后的松弛失败所致。它可能与食管蠕动部分或完全减慢有关。
我们报告一例58岁女性患者,在1年时间内出现吞咽困难、反流及体重显著减轻(11千克)。经胸部和腹部增强计算机断层扫描(CT)、泛影葡胺食管造影及食管测压后,诊断为有症状的贲门失弛缓症合并巨食管。患者拒绝所有微创内镜治疗,直接选择了艾弗·刘易斯(Ivor-Lewis)式食管切除术。在6个月的随访中,患者总体临床状况良好,口服泛影葡胺造影(OGR)显示食管通道良好。
当贲门失弛缓症侵蚀食管壁足以形成巨食管时,患者需要医疗关注。在此阶段,早期微创治疗(即药物治疗、内镜扩张和肌切开术)并不充分,因此需要进行食管手术。在最常见的手术方法中,我们必须提及麦克基翁(McKeown)式食管切除术和威尔金斯(Wilkins)式带结肠袢间置的食管切除术;然而,根据我们的经验,艾弗·刘易斯式经胸内吻合的食管切除术效果极佳,因此可被视为治疗复杂病例的有效选择。
艾弗·刘易斯式经胸内吻合的次全食管切除术治疗贲门失弛缓症合并巨食管有效。