de Bree Remco, Meerkerk Christiaan D A, Halmos Gyorgy B, Mäkitie Antti A, Homma Akihiro, Rodrigo Juan P, López Fernando, Takes Robert P, Vermorken Jan B, Ferlito Alfio
Department of Head and Neck Surgical Oncology, University Medical Center Utrecht, University of Utrecht, Utrecht, Netherlands.
Department of Otorhinolaryngology - Head and Neck Surgery, University Medical Center Groningen, University of Groningen, Groningen, Netherlands.
Front Oncol. 2022 May 12;12:884988. doi: 10.3389/fonc.2022.884988. eCollection 2022.
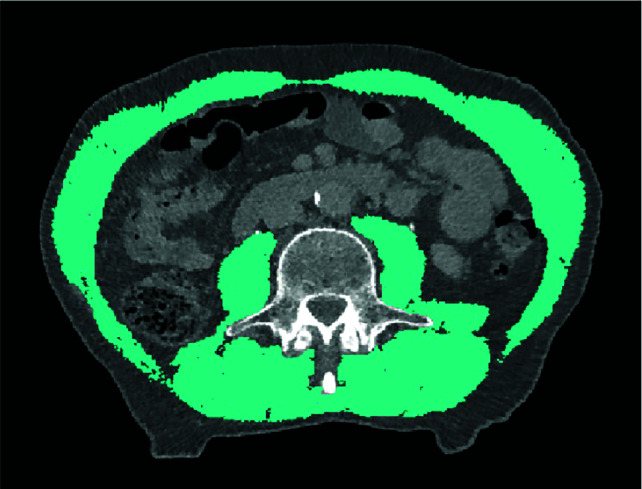
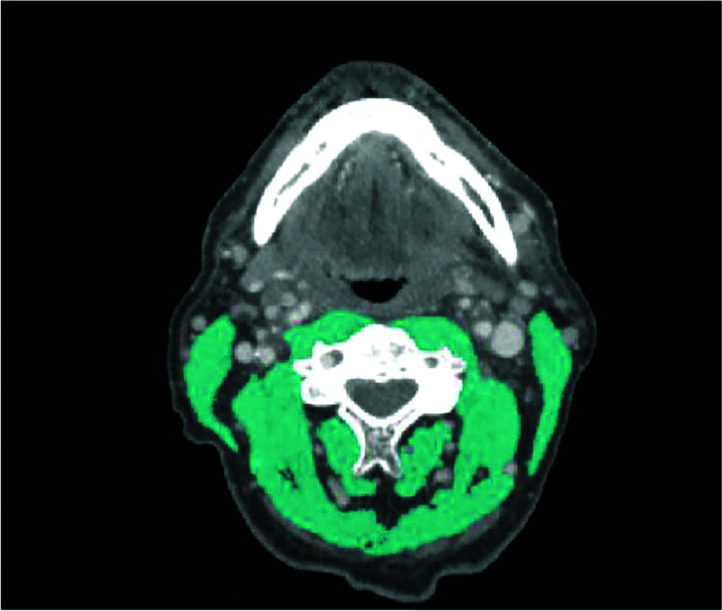
In head and neck cancer (HNC) there is a need for more personalized treatment based on risk assessment for treatment related adverse events (i.e. toxicities and complications), expected survival and quality of life. Sarcopenia, defined as a condition characterized by loss of skeletal muscle mass and function, can predict adverse outcomes in HNC patients. A review of the literature on the measurement of sarcopenia in head and neck cancer patients and its association with frailty was performed. Skeletal muscle mass (SMM) measurement only is often used to determine if sarcopenia is present or not. SMM is most often assessed by measuring skeletal muscle cross-sectional area on CT or MRI at the level of the third lumbar vertebra. As abdominal scans are not always available in HNC patients, measurement of SMM at the third cervical vertebra has been developed and is frequently used. Frailty is often defined as an age-related cumulative decline across multiple physiologic systems, with impaired homeostatic reserve and a reduced capacity of the organism to withstand stress, leading to increased risk of adverse health outcomes. There is no international standard measure of frailty and there are multiple measures of frailty. Both sarcopenia and frailty can predict adverse outcomes and can be used to identify vulnerable patients, select treatment options, adjust treatments, improve patient counselling, improve preoperative nutritional status and anticipate early on complications, length of hospital stay and discharge. Depending on the definitions used for sarcopenia and frailty, there is more or less overlap between both conditions. However, it has yet to be determined if sarcopenia and frailty can be used interchangeably or that they have additional value and should be used in combination to optimize individualized treatment in HNC patients.
在头颈癌(HNC)中,需要根据治疗相关不良事件(即毒性和并发症)、预期生存率和生活质量的风险评估来进行更个性化的治疗。肌肉减少症被定义为以骨骼肌质量和功能丧失为特征的一种状况,它可以预测HNC患者的不良预后。本文对有关头颈癌患者肌肉减少症的测量及其与衰弱的关联的文献进行了综述。仅骨骼肌质量(SMM)测量常被用于确定是否存在肌肉减少症。SMM最常通过在第三腰椎水平的CT或MRI上测量骨骼肌横截面积来评估。由于HNC患者并非总能进行腹部扫描,因此已开发并经常使用在第三颈椎水平测量SMM的方法。衰弱通常被定义为多个生理系统中与年龄相关的累积衰退,体内平衡储备受损,机体承受压力的能力降低,导致不良健康结局的风险增加。目前尚无国际标准的衰弱测量方法,且有多种衰弱测量方法。肌肉减少症和衰弱都可以预测不良预后,可用于识别脆弱患者、选择治疗方案、调整治疗、改善患者咨询、改善术前营养状况以及尽早预测并发症、住院时间和出院情况。根据用于定义肌肉减少症和衰弱的标准,这两种情况之间或多或少存在重叠。然而,肌肉减少症和衰弱是否可以互换使用,或者它们是否具有额外价值,是否应联合使用以优化HNC患者的个体化治疗,仍有待确定。