Moon Jong Youn, Bae Gi Hwan, Jung Jaehun, Shin Dong Hoon
Department of Preventive Medicine, Gachon University College of Medicine, Incheon, Republic of Korea.
Artificial Intelligence and Big-data Convergence Center, Gachon University Gil Medical Center, Incheon, Republic of Korea.
Int J Cardiol Heart Vasc. 2022 Apr 26;40:101037. doi: 10.1016/j.ijcha.2022.101037. eCollection 2022 Jun.
Resuming anticoagulation after an intracranial hemorrhage (ICH) poses a clinical conundrum. The absence of relevant guidelines has led to wide variations in the decision on resuming anticoagulation therapies after ICH. This study aimed to evaluate the risks of an anticoagulation therapy on severe thrombotic events (STE) and severe hemorrhage events (SHE) in Korea and compare the effects of novel direct oral anticoagulants (NOACs) and warfarin in patients with AF.
This study was performed using the Korean national health insurance claims data obtained between 2002 and 2017 from individuals who had recently survived an ICH with comorbid AF. The endpoints of this study were STE and SHE. Anticoagulants, antiplatelet agents, and non-antithrombotic users were analyzed for survival with propensity score matching.
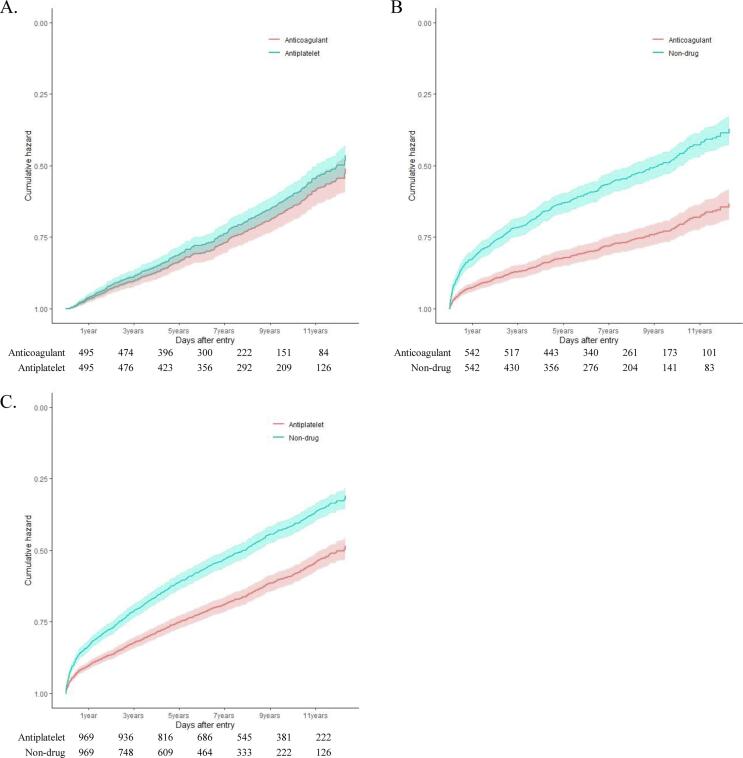
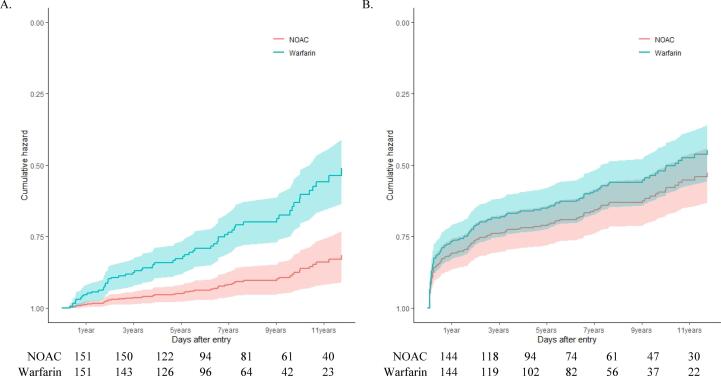
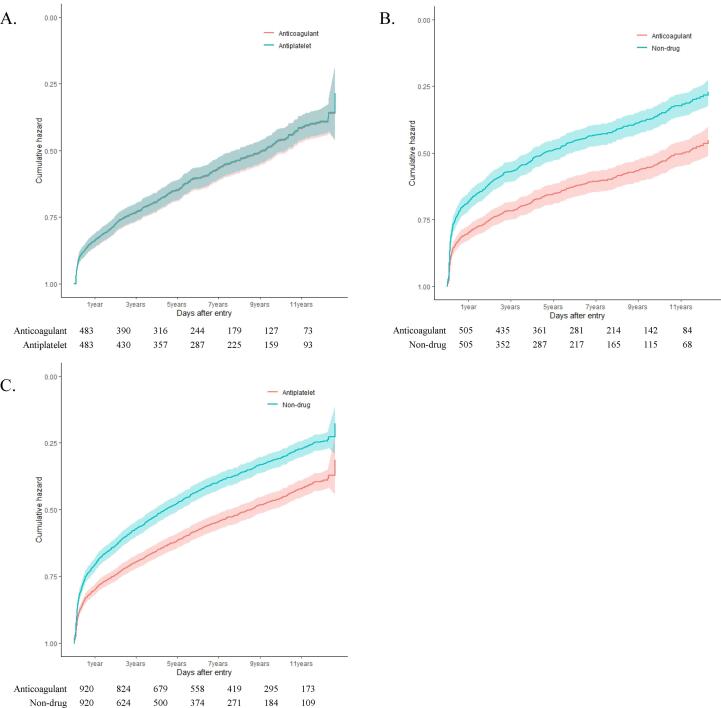
Among the 4,964 participants analyzed, 878 (17.7%) and 2,070 (41.7%) used anticoagulant and antiplatelet agents, respectively. Anticoagulant (hazard ratio [HR] for STE: 0.385, < 0.0001; HR for SHE: 0.578, < 0.0001) or antiplatelet users (HR for STE: 0.545, < 0.0001; HR for SHE: 0.637, < 0.0001) had a lower risk of STE and SHE than non-antithrombotic users. Anticoagulation 6-8 weeks post-ICH showed a tendency of the lowest risk of all-cause mortality (HR: 0.614, P = 0.0552). However, there was no difference in the risk between the anticoagulant and antiplatelet users. Further, NOACs were associated with a lower risk of STEs than warfarin (HR, 0.263; < 0.0001).
Our results showed that in patients with AF, resuming anticoagulants and antiplatelets after ICH improved the STEs and SHEs. Further, NOAC had additional benefits as compared to warfarin.
颅内出血(ICH)后恢复抗凝治疗是一个临床难题。由于缺乏相关指南,ICH后恢复抗凝治疗的决策存在很大差异。本研究旨在评估韩国抗凝治疗对严重血栓事件(STE)和严重出血事件(SHE)的风险,并比较新型直接口服抗凝剂(NOACs)和华法林对房颤患者的影响。
本研究使用了2002年至2017年期间从近期患有合并房颤的ICH幸存者中获得的韩国国民健康保险理赔数据。本研究的终点是STE和SHE。通过倾向评分匹配分析抗凝剂、抗血小板药物和非抗血栓治疗使用者的生存率。
在分析的4964名参与者中,分别有878名(17.7%)和2070名(41.7%)使用了抗凝剂和抗血小板药物。抗凝剂使用者(STE的风险比[HR]:0.385,<0.0001;SHE的HR:0.578,<0.0001)或抗血小板药物使用者(STE的HR:0.545,<0.0001;SHE的HR:0.637,<0.0001)发生STE和SHE的风险低于非抗血栓治疗使用者。ICH后6-8周进行抗凝治疗显示全因死亡率风险有最低的趋势(HR:0.614,P=0.0552)。然而,抗凝剂使用者和抗血小板药物使用者之间的风险没有差异。此外,与华法林相比,NOACs发生STEs的风险更低(HR,0.263;<0.0001)。
我们的结果表明,在房颤患者中,ICH后恢复使用抗凝剂和抗血小板药物可改善STE和SHE。此外,与华法林相比,NOAC有额外的益处。