Department of Pharmacy National Taiwan University Hospital Taipei Taiwan.
School of Pharmacy College of MedicineNational Taiwan University Taipei Taiwan.
J Am Heart Assoc. 2022 Mar 15;11(6):e022849. doi: 10.1161/JAHA.121.022849. Epub 2022 Mar 4.
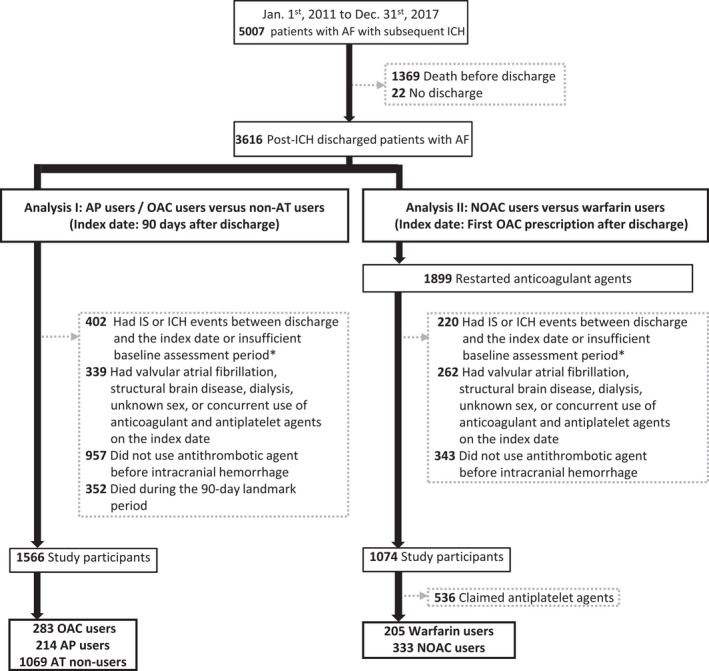
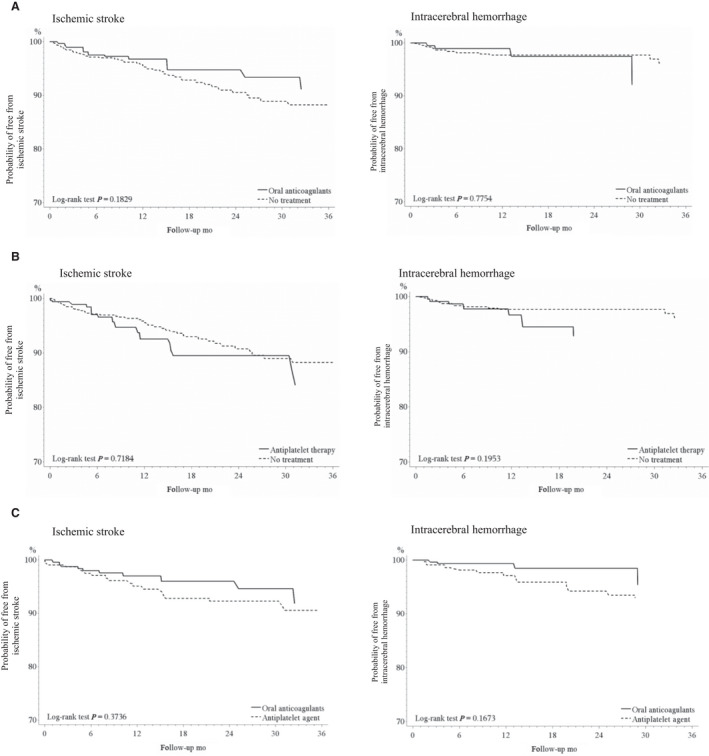
Background To investigate the effectiveness and safety of withholding or restarting antithrombotic agents, and different antithrombotic therapies among patients with atrial fibrillation post-intracranial hemorrhage. Methods and Results This is a nationwide retrospective cohort study involving patients with atrial fibrillation receiving antithrombotic therapies who subsequently developed intracranial hemorrhage between January 1, 2011 and December 31, 2017. The risk of ischemic stroke (IS), recurrent intracerebral hemorrhage (ICH), and all-cause mortality were investigated between patients receiving no treatment versus patients reinitiating oral anticoagulants (OACs) or antiplatelet agents, and warfarin versus non-vitamin K antagonist OACs. We applied inverse probability of treatment weighting to balance the baseline characteristics and Cox proportional hazards model to estimate the hazard ratios (HRs) of different outcomes of interest. Compared with no treatment, OACs reduced the risk of IS (HR, 0.61; 0.42-0.89), without increase in the risk of ICH (1.15, 0.66-2.02); antiplatelet agent users showed a similar risk of IS (1.13, 0.81-1.56) and increased risk of ICH (1.81, 1.07-3.04). Use of OACs or antiplatelet agents did not reduce the risk of all-cause mortality (0.85, 0.72-1.01; and 0.88, 0.75-1.03, respectively). Compared with warfarin, non-vitamin K antagonist OAC users showed a similar risk of IS (0.92, 0.50-1.70), non-significantly reduced risk of ICH (0.53, 0.22-1.30), and significantly reduced all-cause mortality (0.60, 0.43-0.84). Conclusions OACs are recommended in patients with atrial fibrillation and intracranial hemorrhage because they reduced the risk of IS with no increase in the risk of subsequent ICH. Non-vitamin K antagonist OACs are recommended over warfarin owing to their survival benefits.
研究颅内出血后房颤患者抗栓药物的停用或重新使用以及不同抗栓治疗的有效性和安全性。
这是一项全国性的回顾性队列研究,纳入了 2011 年 1 月 1 日至 2017 年 12 月 31 日期间接受抗栓治疗后发生颅内出血的房颤患者。研究比较了未治疗患者与重新开始使用口服抗凝剂(OACs)或抗血小板药物、华法林与非维生素 K 拮抗剂 OACs 患者之间的缺血性卒中(IS)、复发性颅内出血(ICH)和全因死亡率风险。采用逆概率处理加权法(inverse probability of treatment weighting, IPTW)平衡基线特征,采用 Cox 比例风险模型(Cox proportional hazards model)估计不同结局的风险比(hazard ratio,HR)。与未治疗相比,OACs 降低了 IS 风险(HR 0.61,0.42-0.89),ICH 风险无增加(1.15,0.66-2.02);抗血小板药物使用者的 IS 风险相似(1.13,0.81-1.56),ICH 风险增加(1.81,1.07-3.04)。OACs 或抗血小板药物的使用并不能降低全因死亡率风险(0.85,0.72-1.01;0.88,0.75-1.03)。与华法林相比,非维生素 K 拮抗剂 OAC 使用者的 IS 风险相似(0.92,0.50-1.70),ICH 风险非显著降低(0.53,0.22-1.30),全因死亡率显著降低(0.60,0.43-0.84)。
颅内出血后房颤患者推荐使用 OACs,因其降低了 IS 风险,且不增加随后 ICH 的风险。非维生素 K 拮抗剂 OAC 优于华法林,因其有生存获益。