The University of Manchester and The Christie NHS Foundation Trust, Manchester, UK.
Centre for Trials Research, Cardiff University, Cardiff, UK.
Lancet Oncol. 2022 Jul;23(7):851-864. doi: 10.1016/S1470-2045(22)00284-4. Epub 2022 Jun 4.
Capivasertib, an AKT inhibitor, added to fulvestrant, was previously reported to improve progression-free survival in women with aromatase inhibitor-resistant oestrogen receptor (ER)-positive, HER2-negative advanced breast cancer. The benefit appeared to be independent of the phosphoinositide 3-kinase (PI3K)/AKT/phosphatase and tensin homologue (PTEN) pathway alteration status of tumours, as ascertained using assays available at the time. Here, we report updated progression-free survival and overall survival results, and a prespecified examination of the effect of PI3K/AKT/PTEN pathway alterations identified by an expanded genetic testing panel on treatment outcomes.
This randomised, multicentre, double-blind, placebo-controlled, phase 2 trial recruited postmenopausal adult women aged at least 18 years with ER-positive, HER2-negative, metastatic or locally advanced inoperable breast cancer and an Eastern Cooperative Oncology Group performance status of 0-2, who had relapsed or progressed on an aromatase inhibitor, from across 19 hospitals in the UK. Participants were randomly assigned (1:1) to receive intramuscular fulvestrant 500 mg (day 1) every 28 days (plus a 500 mg loading dose on day 15 of cycle 1) with either capivasertib 400 mg or matching placebo, orally twice daily on an intermittent weekly schedule of 4 days on and 3 days off, starting on cycle 1 day 15. Treatment continued until disease progression, unacceptable toxicity, loss to follow-up, or withdrawal of consent. Treatment was allocated by an interactive web-response system using a minimisation method (with a 20% random element) and the following minimisation factors: measurable or non-measurable disease, primary or secondary aromatase inhibitor resistance, PIK3CA status, and PTEN status. The primary endpoint was progression-free survival in the intention-to-treat population. Secondary endpoints shown in this Article were overall survival and safety in the intention-to-treat population, and the effect of tumour PI3K/AKT/PTEN pathway status identified by an expanded testing panel that included next-generation sequencing assays. Recruitment is complete. The trial is registered with ClinicalTrials.gov, number NCT01992952.
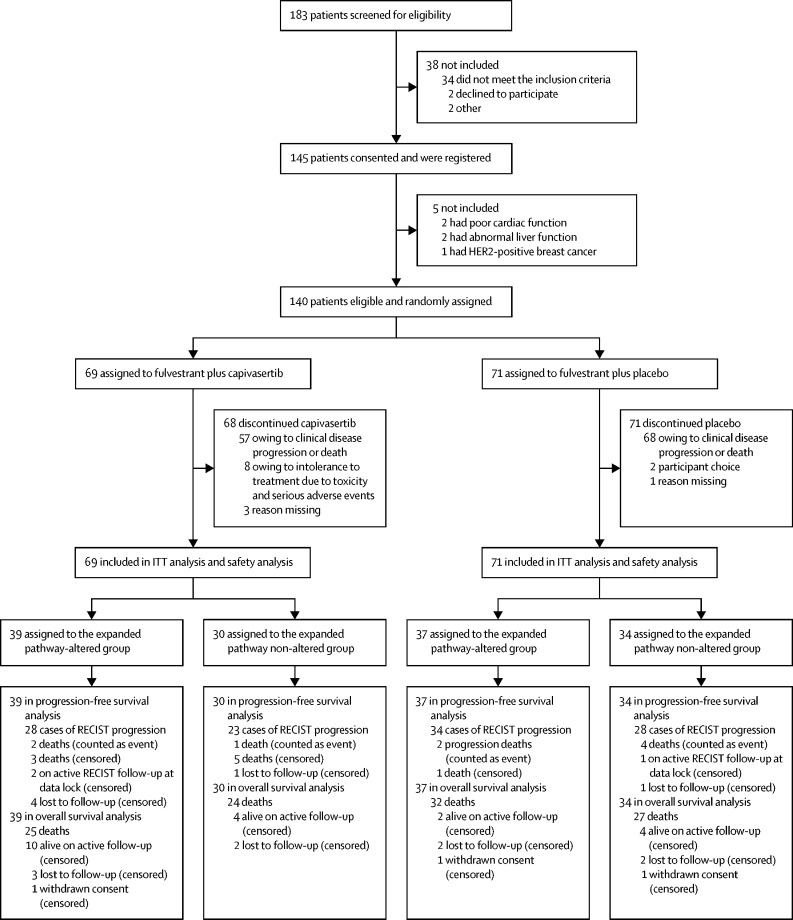
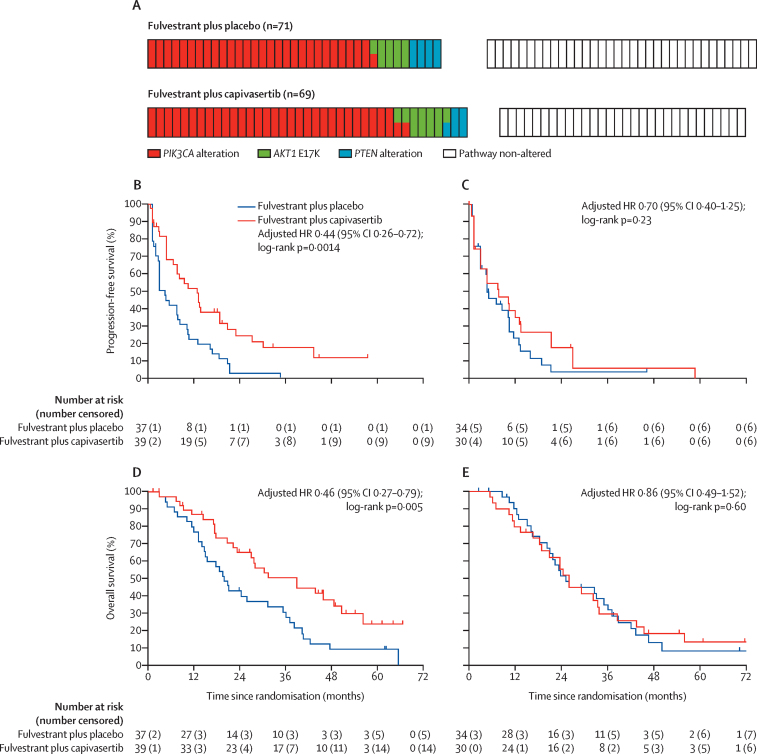
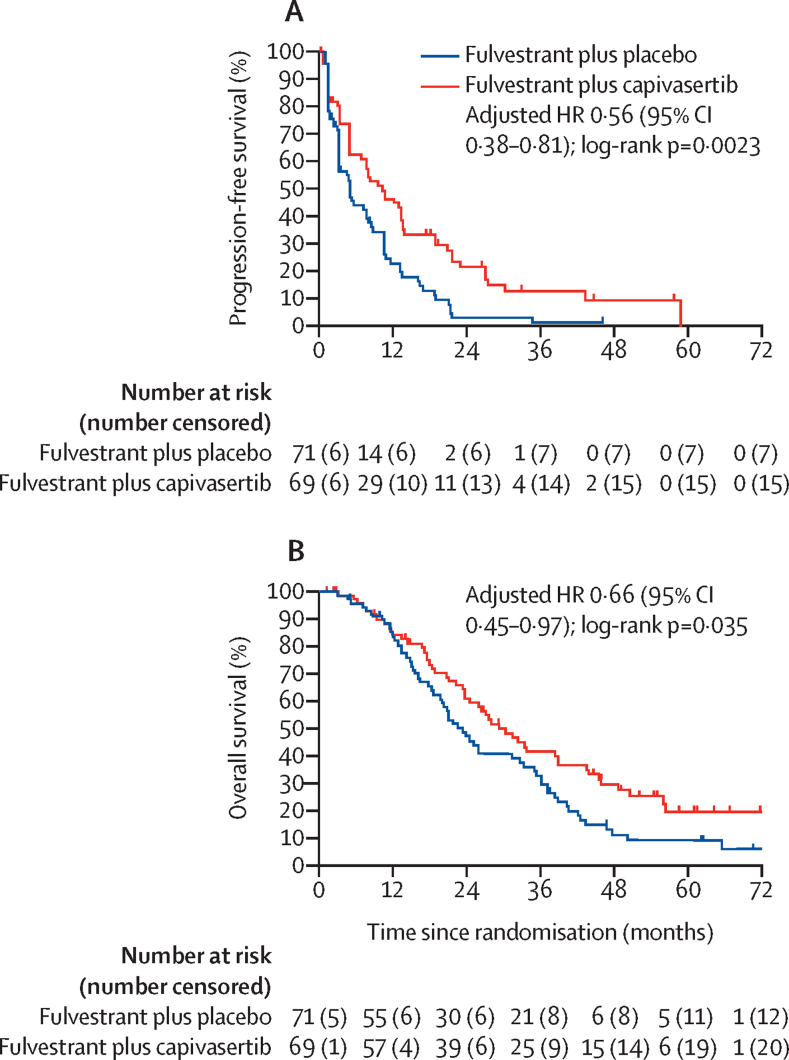
Between March 16, 2015, and March 6, 2018, 183 participants were screened for eligibility and 140 (77%) were randomly assigned to receive fulvestrant plus capivasertib (n=69) or fulvestrant plus placebo (n=71). Median follow-up at the data cut-off of Nov 25, 2021, was 58·5 months (IQR 45·9-64·1) for participants treated with fulvestrant plus capivasertib and 62·3 months (IQR 62·1-70·3) for fulvestrant plus placebo. Updated median progression-free survival was 10·3 months (95% CI 5·0-13·4) in the group receiving fulvestrant plus capivasertib compared with 4·8 months (3·1-7·9) for fulvestrant plus placebo (adjusted hazard ratio [HR] 0·56 [95% CI 0·38-0·81]; two-sided p=0·0023). Median overall survival in the capivasertib versus placebo groups was 29·3 months (95% CI 23·7-39·0) versus 23·4 months (18·7-32·7; adjusted HR 0·66 [95% CI 0·45-0·97]; two-sided p=0·035). The expanded biomarker panel identified an expanded pathway-altered subgroup that contained 76 participants (54% of the intention-to-treat population). Median progression-free survival in the expanded pathway-altered subgroup for participants receiving capivasertib (n=39) was 12·8 months (95% CI 6·6-18·8) compared with 4·6 months (2·8-7·9) in the placebo group (n=37; adjusted HR 0·44 [95% CI 0·26-0·72]; two-sided p=0·0014). Median overall survival for the expanded pathway-altered subgroup receiving capivasertib was 38·9 months (95% CI 23·3-50·7) compared with 20·0 months (14·8-31·4) for those receiving placebo (adjusted HR 0·46 [95% CI 0·27-0·79]; two-sided p=0·0047). By contrast, there were no statistically significant differences in progression-free or overall survival in the expanded pathway non-altered subgroup treated with capivasertib (n=30) versus placebo (n=34). One additional serious adverse event (pneumonia) in the capivasertib group had occurred subsequent to the primary analysis. One death, due to atypical pulmonary infection, was assessed as possibly related to capivasertib treatment.
Updated FAKTION data showed that capivasertib addition to fulvestrant extends the survival of participants with aromatase inhibitor-resistant ER-positive, HER2-negative advanced breast cancer. The expanded biomarker testing suggested that capivasertib predominantly benefits patients with PI3K/AKT/PTEN pathway-altered tumours. Phase 3 data are needed to substantiate the results, including in patients with previous CDK4/6 inhibitor exposure who were not included in the FAKTION trial.
AstraZeneca and Cancer Research UK.
先前的研究表明,AKT 抑制剂卡培他滨联合氟维司群可改善芳香酶抑制剂耐药的雌激素受体(ER)阳性、HER2 阴性晚期乳腺癌患者的无进展生存期。该获益似乎与肿瘤磷酸肌醇 3-激酶(PI3K)/AKT/磷酸酶和张力蛋白同源物(PTEN)通路改变状态无关,因为当时可用的检测方法证实了这一点。在此,我们报告了更新的无进展生存期和总生存期结果,并对使用扩展遗传检测面板确定的 PI3K/AKT/PTEN 通路改变对治疗结果的影响进行了预设检查。
这是一项随机、多中心、双盲、安慰剂对照的 2 期临床试验,在英国 19 家医院招募了至少 18 岁的绝经后成年女性,这些患者患有转移性或局部晚期不可手术的 ER 阳性、HER2 阴性乳腺癌,ECOG 体能状态为 0-2 分,且在接受芳香酶抑制剂治疗后复发或进展。参与者以 1:1 的比例随机分配(1:1)接受肌肉注射氟维司群 500mg(第 1 天),每 28 天一次(第 1 个周期的第 15 天给予 500mg 负荷剂量),同时接受卡培他滨 400mg 或匹配安慰剂,每日口服两次,每周间歇给药 4 天,停药 3 天,从第 1 个周期第 15 天开始。治疗持续到疾病进展、无法耐受毒性、失访或退出同意。治疗方案通过交互式网络响应系统进行分配,该系统使用最小化方法(随机元素占 20%)和以下最小化因素:可测量或不可测量的疾病、原发性或继发性芳香酶抑制剂耐药、PIK3CA 状态和 PTEN 状态。主要终点是意向治疗人群的无进展生存期。本文中显示的次要终点是意向治疗人群的总生存期和安全性,以及使用包括下一代测序检测在内的扩展检测面板确定的肿瘤 PI3K/AKT/PTEN 通路状态的影响。招募工作已经完成。该试验在 ClinicalTrials.gov 注册,编号为 NCT01992952。
2015 年 3 月 16 日至 2018 年 3 月 6 日,筛选了 183 名患者以确定其是否符合入组条件,其中 140 名(77%)被随机分配接受氟维司群联合卡培他滨(n=69)或氟维司群联合安慰剂(n=71)治疗。截至 2021 年 11 月 25 日数据截止时,氟维司群联合卡培他滨组的中位随访时间为 58.5 个月(IQR 45.9-64.1),氟维司群联合安慰剂组为 62.3 个月(IQR 62.1-70.3)。更新后的中位无进展生存期为氟维司群联合卡培他滨组的 10.3 个月(95%CI 5.0-13.4),而氟维司群联合安慰剂组为 4.8 个月(3.1-7.9)(调整后的 HR 0.56 [95%CI 0.38-0.81];双侧 p=0.0023)。卡培他滨组与安慰剂组的中位总生存期分别为 29.3 个月(95%CI 23.7-39.0)和 23.4 个月(18.7-32.7)(调整后的 HR 0.66 [95%CI 0.45-0.97];双侧 p=0.035)。扩展的生物标志物检测面板确定了一个包含 76 名患者(意向治疗人群的 54%)的扩展通路改变亚组。卡培他滨组中接受卡培他滨治疗的患者(n=39)的中位无进展生存期为 12.8 个月(95%CI 6.6-18.8),而安慰剂组(n=37)为 4.6 个月(2.8-7.9)(调整后的 HR 0.44 [95%CI 0.26-0.72];双侧 p=0.0014)。接受卡培他滨治疗的扩展通路改变亚组的中位总生存期为 38.9 个月(95%CI 23.3-50.7),而安慰剂组为 20.0 个月(14.8-31.4)(调整后的 HR 0.46 [95%CI 0.27-0.79];双侧 p=0.0047)。相比之下,在接受卡培他滨治疗的扩展通路未改变亚组中,无进展生存期或总生存期在卡培他滨组(n=30)和安慰剂组(n=34)之间没有统计学上的显著差异。卡培他滨组还发生了 1 例(肺炎)与主要分析后发生的额外严重不良事件。1 例死亡(非典型性肺部感染)被评估为可能与卡培他滨治疗相关。
更新的 FAKTION 数据显示,卡培他滨联合氟维司群可延长芳香酶抑制剂耐药的 ER 阳性、HER2 阴性晚期乳腺癌患者的生存。扩展的生物标志物检测表明,卡培他滨主要使 PI3K/AKT/PTEN 通路改变的肿瘤获益。需要进行 3 期数据研究来证实这些结果,包括之前未接受 CDK4/6 抑制剂治疗的患者。
阿斯利康和英国癌症研究基金会。