Chau Oi-Wai, Fakir Hatim, Lock Michael, Dinniwell Robert, Perera Francisco, Erickson Abigail, Gaede Stewart
Physics and Engineering, London Regional Cancer Program, London, CAN.
Radiation Oncology, Schulich School of Medicine and Dentistry, Western University, London, CAN.
Cureus. 2022 May 6;14(5):e24777. doi: 10.7759/cureus.24777. eCollection 2022 May.
Adjuvant whole-breast radiotherapy (RT) is a significant part of the standard of care treatment after breast cancer (BC) conserving surgery. Modern techniques including intensity-modulated radiation therapy (IMRT) and volumetric-modulated arc therapy (VMAT) have constituted to better target coverage and critical organs sparing. However, BC survivors are at risk of developing radiation-induced cardiac toxicity. Hence, deep-inspiration breath-hold (DIBH) techniques have been implemented at many centers to further reduce cardiac exposure but require compliance. 4D-CT robust optimization can account for heart intrafractional motion per breathing phase. The optimization has been explored in cardiac sparing of breast IMRT compared to DIBH in a small sample size but has not been evaluated in substructures sparing, nor in VMAT. To provide patients who are not compliant to breath-hold with an optimal treatment approach, various heart sparing techniques need to be evaluated for statistical significance and clinical feasibility.
This retrospective study aimed to provide an extensive dosimetric heart sparing comparison of free-breathing, 4D-CT-based treatment planning, including robust optimization with DIBH-based treatment planning. Combinations of forward and inverse IMRT and VMAT are also considered.
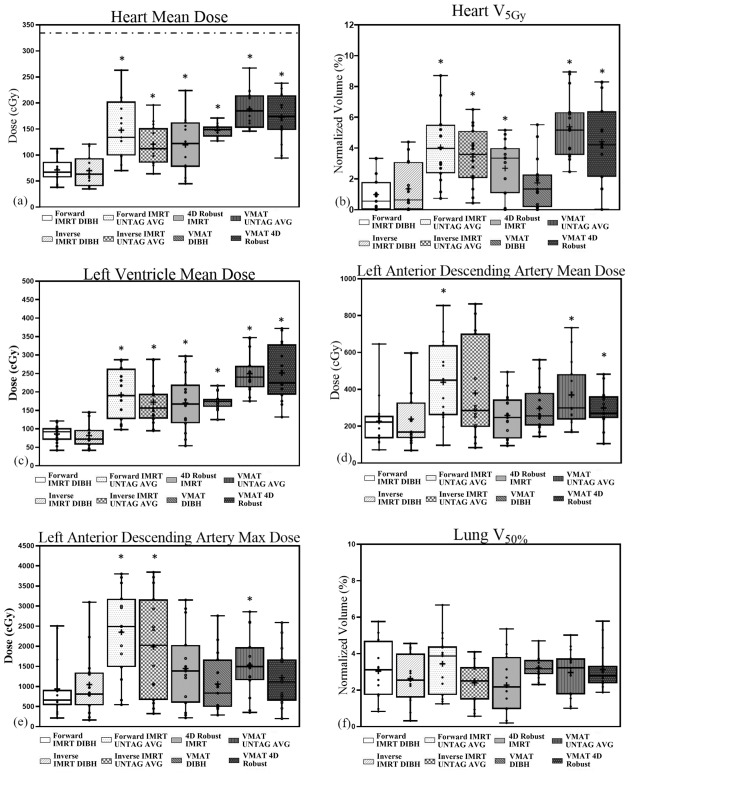
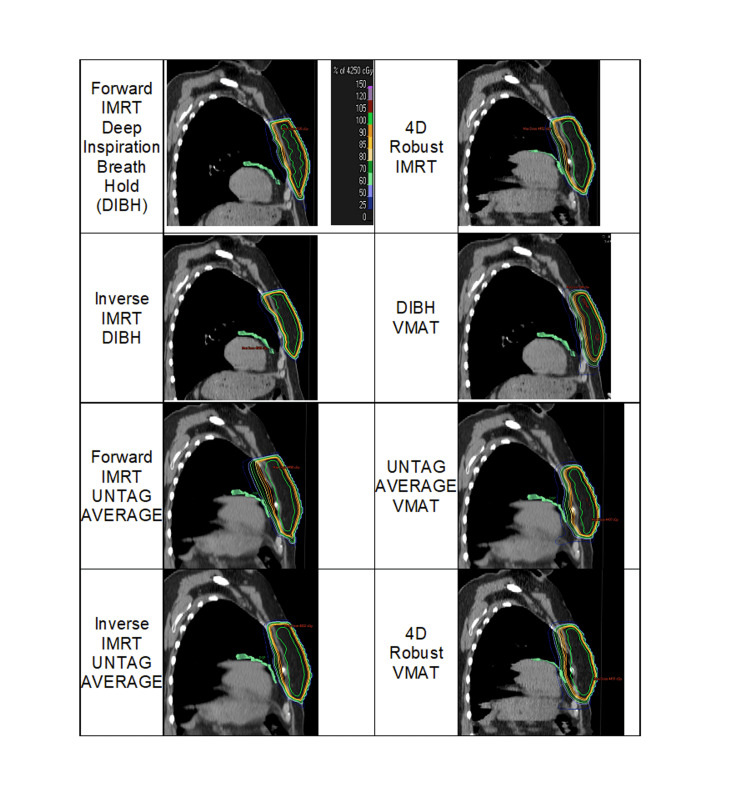
Fifteen early stage left-sided BC standard treatment plans were selected. Breast, lung, left anterior descending artery (LAD), left ventricle (LV), and the whole heart were contoured on each 4D-CT phase and DIBH CT dataset. Each treatment plan was optimized using forward/inverse IMRT and VMAT on the following CT datasets: DIBH, average 4D-CT, and the complete 4D-CT dataset needed for robust optimization. Dose-volume histograms were used to compare VHeart, mean heart dose, mean and max LAD dose, mean LV dose, and VLung.
All RT techniques assessed including 4D robust optimization were clinically feasible. Statistically significant differences in mean heart, LAD and LV dose, max LAD dose, and VHeart (p < 0.01) but no difference in VLung (p = 0.29) were found between different techniques. IMRT DIBH achieved the optimal cardiac and substructure sparing among treatment plans. 4D robust IMRT had significantly greater mean heart and LV dose than DIBH IMRT (p ≤ 0.01), except LAD dose. Among free-breathing methods, no difference in all cardiac and substructure dose parameters was observed (p > 0.2) in comparing forward and inverse IMRT with average 4D-CT, inverse average 4D-CT, and 4D robust with IMRT, and between average 4D-CT VMAT and 4D robust VMAT. Only VHeart and mean LV dose were significantly greater in 4D robust VMAT (p < 0.01) compared to DIBH VMAT. Mean heart and LV doses were significantly reduced (p < 0.01) in DIBH IMRT compared to DIBH VMAT. Moreover, mean heart and LV dose, VHeart were significantly reduced in inverse IMRT average 4D-CT compared to average 4D-CT VMAT (p < 0.02) and in 4D robust IMRT compared to 4D robust VMAT (p < 0.04).
This study demonstrated the clinical feasibility of 4D robust optimization in limiting the cardiac and substructures dose during free-breathing RT with both IMRT/VMAT for patients who are not compliant with breath-hold RT. However, this study also presents that 4D robust optimization can reduce LAD dose but not fully outperform DIBH or conventional 4D-CT-based planning with IMRT/VMAT in heart sparing in treating early staged left-sided BC patients.
辅助性全乳放疗(RT)是保乳手术后标准治疗方案的重要组成部分。包括调强放射治疗(IMRT)和容积调强弧形治疗(VMAT)在内的现代技术有助于更好地实现靶区覆盖并保护关键器官。然而,乳腺癌幸存者有发生放射性心脏毒性的风险。因此,许多中心已采用深吸气屏气(DIBH)技术以进一步减少心脏受照剂量,但该技术需要患者配合。4D-CT稳健优化可考虑每个呼吸阶段心脏的分次内运动。在小样本研究中,已对IMRT心脏保护方面的4D-CT稳健优化与DIBH进行了比较,但尚未在亚结构保护以及VMAT中进行评估。为给不配合屏气的患者提供最佳治疗方案,需要评估各种心脏保护技术的统计学意义和临床可行性。
本回顾性研究旨在对自由呼吸、基于4D-CT的治疗计划(包括基于DIBH的治疗计划的稳健优化)进行广泛的心脏剂量学保护比较。同时也考虑了正向和逆向IMRT与VMAT的组合。
选择15例左侧早期乳腺癌的标准治疗计划。在每个4D-CT相位和DIBH CT数据集中勾勒出乳房、肺、左前降支动脉(LAD)、左心室(LV)和全心的轮廓。每个治疗计划在以下CT数据集上使用正向/逆向IMRT和VMAT进行优化:DIBH、平均4D-CT以及稳健优化所需的完整4D-CT数据集。使用剂量体积直方图比较心脏体积(VHeart)、平均心脏剂量、平均和最大LAD剂量、平均LV剂量以及肺体积(VLung)。
所有评估的放疗技术包括4D稳健优化在临床上都是可行的。不同技术之间在平均心脏、LAD和LV剂量、最大LAD剂量以及VHeart方面存在统计学显著差异(p < 0.01),但在VLung方面无差异(p = 0.29)。在治疗计划中,IMRT DIBH实现了最佳的心脏和亚结构保护。4D稳健IMRT的平均心脏和LV剂量比DIBH IMRT显著更高(p ≤ 0.01),LAD剂量除外。在自由呼吸方法中,比较正向和逆向IMRT与平均4D-CT、逆向平均4D-CT以及4D稳健IMRT时,所有心脏和亚结构剂量参数均无差异(p > 0.2),平均4D-CT VMAT与4D稳健VMAT之间也无差异。与DIBH VMAT相比,仅4D稳健VMAT中的VHeart和平均LV剂量显著更高(p < 0.01)。与DIBH VMAT相比,DIBH IMRT中的平均心脏和LV剂量显著降低(p < 0.01)。此外,与平均4D-CT VMAT相比,逆向IMRT平均4D-CT中的平均心脏和LV剂量、VHeart显著降低(p < 0.02),与4D稳健VMAT相比,4D稳健IMRT中的这些参数也显著降低(p < 0.04)。
本研究证明了4D稳健优化在不配合屏气放疗的患者进行自由呼吸放疗时限制心脏和亚结构剂量方面的临床可行性。然而,本研究也表明,在治疗早期左侧乳腺癌患者时,4D稳健优化可降低LAD剂量,但在心脏保护方面不能完全优于DIBH或基于传统4D-CT的IMRT/VMAT计划。