Block Valerie J, Waliman Matthew, Xie Zhendong, Akula Amit, Bove Riley, Pletcher Mark J, Marcus Gregory M, Olgin Jeffrey E, Cree Bruce A C, Gelfand Jeffrey M, Henry Roland G
Department of Neurology, University of California San Francisco (UCSF) Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA, United States.
Department of Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, CA, United States.
Front Neurol. 2022 May 23;13:860008. doi: 10.3389/fneur.2022.860008. eCollection 2022.
Ambulatory disability is common in people with multiple sclerosis (MS). Remote monitoring using average daily step count (STEPS) can assess physical activity (activity) and disability in MS. STEPS correlates with conventional metrics such as the expanded disability status scale (Expanded Disability Status Scale; EDSS), Timed-25 Foot walk (T25FW) and timed up and go (TUG). However, while STEPS as a summative measure characterizes the number of steps taken over a day, it does not reflect variability and intensity of activity.
Novel analytical methods were developed to describe how individuals spends time in various activity levels (e.g., continuous low versus short bouts of high) and the proportion of time spent at each activity level.
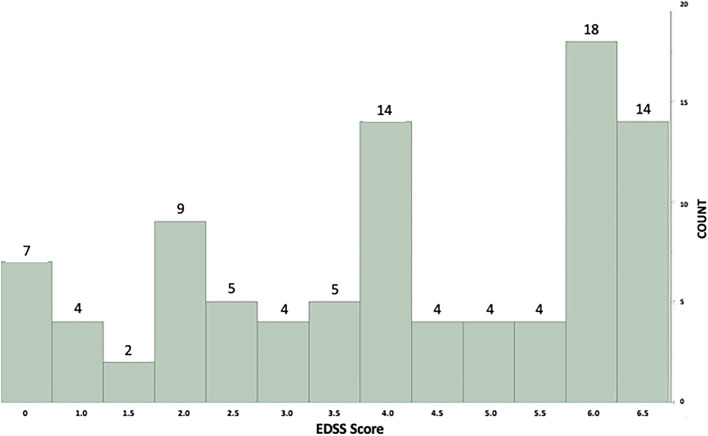
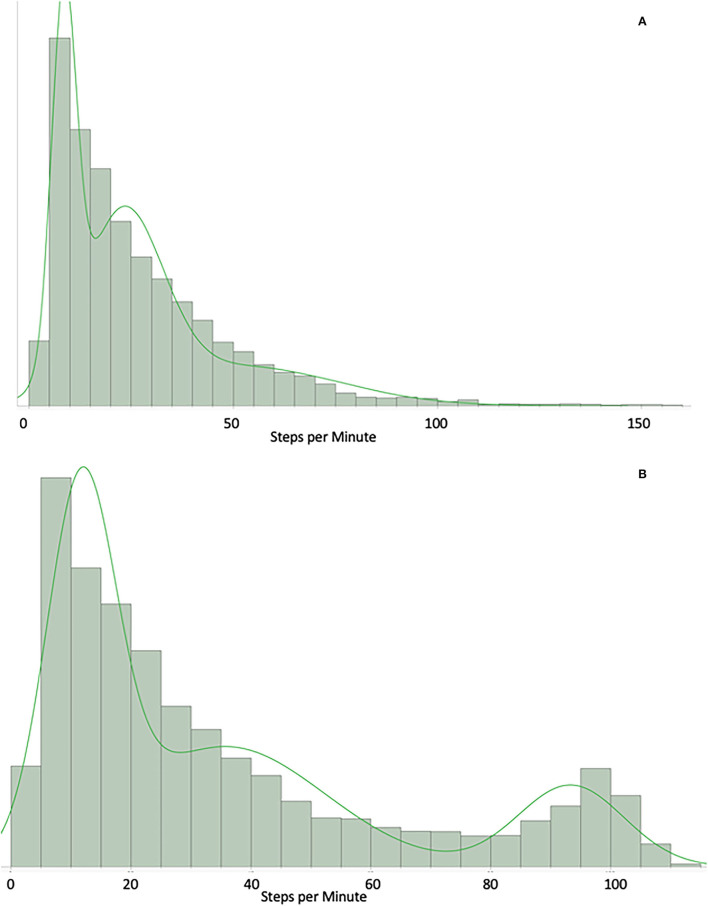
94 people with MS spanning the range of ambulatory impairment (unaffected to requiring bilateral assistance) were recruited into FITriMS study and asked to wear a Fitbit continuously for 1-year. Parametric distributions were fit to minute-by-minute step data. Adjusted R values for regressions between distributional fit parameters and STEPS with EDSS, TUG, T25FW and the patient-reported 12-item MS Walking scale (MSWS-12) were calculated over the first 4-weeks, adjusting for sex, age and disease duration.
Distributional fits determined that the best statistically-valid model across all subjects was a 3-compartment Gaussian Mixture Model (GMM) that characterizes the step behavior within 3 levels of activity: high, moderate and low. The correlation of GMM parameters for baseline step count measures with clinical assessments was improved when compared with STEPS (adjusted R values GMM vs. STEPS: TUG: 0.536 vs. 0.419, T25FW: 0.489 vs. 0.402, MSWS-12: 0.383 vs. 0.378, EDSS: 0.557 vs. 0.465). The GMM correlated more strongly (Kruskal-Wallis: = 0.0001) than STEPS and gave further information not included in STEPS.
Individuals' step distributions follow a 3-compartment GMM that better correlates with clinic-based performance measures compared with STEPS. These data support the existence of high-moderate-low levels of activity. GMM provides an interpretable framework to better understand the association between different levels of activity and clinical metrics and allows further analysis of walking behavior that takes step distribution and proportion of time at three levels of intensity into account.
行走功能障碍在多发性硬化症(MS)患者中很常见。使用平均每日步数(STEPS)进行远程监测可以评估MS患者的身体活动(活动量)和功能障碍情况。STEPS与传统指标相关,如扩展残疾状态量表(Expanded Disability Status Scale;EDSS)、25英尺步行时间(T25FW)和起立行走测试(TUG)。然而,虽然STEPS作为一种汇总测量方法可以表征一天内行走的步数,但它并不能反映活动的变异性和强度。
开发新的分析方法来描述个体在不同活动水平(例如,持续低强度与短时间高强度)下的时间分配情况以及在每个活动水平上花费的时间比例。
94名MS患者(涵盖从无行走功能障碍到需要双侧辅助的不同程度)被纳入FITriMS研究,并被要求连续佩戴Fitbit设备1年。对逐分钟的步数数据拟合参数分布。在最初的4周内,计算分布拟合参数与STEPS、EDSS、TUG、T25FW以及患者报告的12项MS步行量表(MSWS - 12)之间回归的调整R值,并对性别、年龄和病程进行校正。
分布拟合确定,对所有受试者而言,统计有效性最佳的模型是一个三成分高斯混合模型(GMM),该模型可表征三个活动水平(高、中、低)下的步数行为。与STEPS相比,基线步数测量的GMM参数与临床评估的相关性有所提高(GMM与STEPS的调整R值比较:TUG:0.536对0.419,T25FW:0.489对0.402,MSWS - 12:0.383对0.378,EDSS:0.557对0.465)。GMM的相关性比STEPS更强(Kruskal - Wallis检验:P = 0.0001),并提供了STEPS未包含的更多信息。
个体的步数分布遵循三成分GMM,与基于临床的性能指标相比,它与这些指标的相关性更好。这些数据支持存在高、中、低水平的活动。GMM提供了一个可解释的框架,以更好地理解不同活动水平与临床指标之间的关联,并允许对考虑了步数分布和三个强度水平下时间比例的步行行为进行进一步分析。