Department of General, Visceral and Thoracic Surgery, Hospital of Worms, Gabriel-von-Seidl-Strasse 81, 67550, Worms, Germany.
Department of General, Visceral, Thoracic, Transplant and Pediatric Surgery, University Hospital of Giessen, Rudolf-Buchheim-Strasse 7, 35390, Giessen, Germany.
Langenbecks Arch Surg. 2022 Nov;407(7):2915-2927. doi: 10.1007/s00423-022-02576-8. Epub 2022 Jun 9.
Right colectomy (RC) is a frequently performed procedure. Beneath standard conventional open surgery (COS), various minimally invasive techniques had been introduced. Several advantages had recently been described for robotic approaches over COS or conventional laparoscopy. Nevertheless, novel minimally invasive techniques require continuous benchmarking against standard COS to gain maximum patient safety. Bowel dysfunction is a frequent problem after RC. Together with general complication rates postoperative bowel recovery are used as surrogate parameters for postoperative patient outcome in this study.
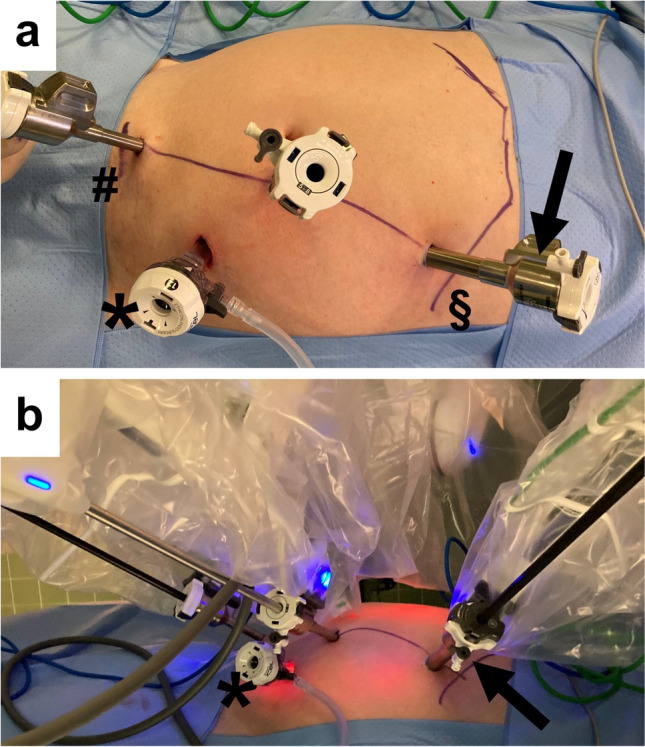
Retrospective, 10-year single-center analysis of consecutive patients who underwent sequentially either COS (n = 22), robotic-assisted (ECA: n = 39), or total robotic surgery (ICA: n = 56) for oncologic RC was performed.
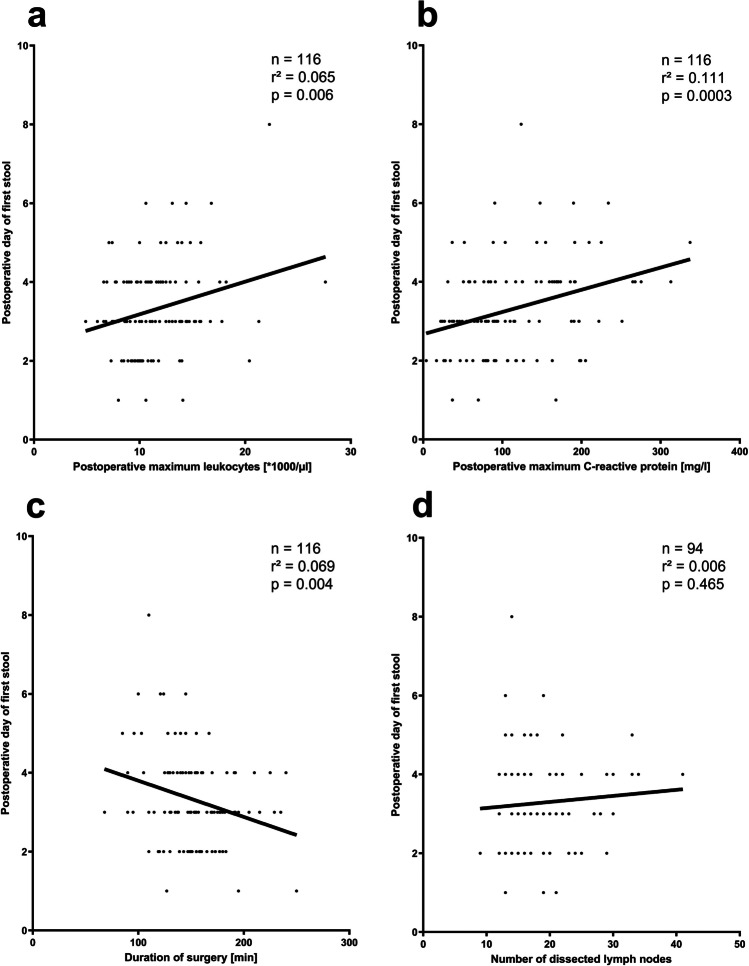
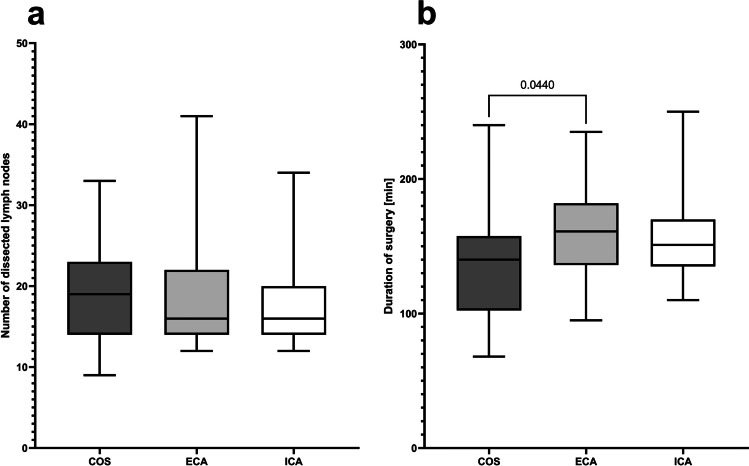
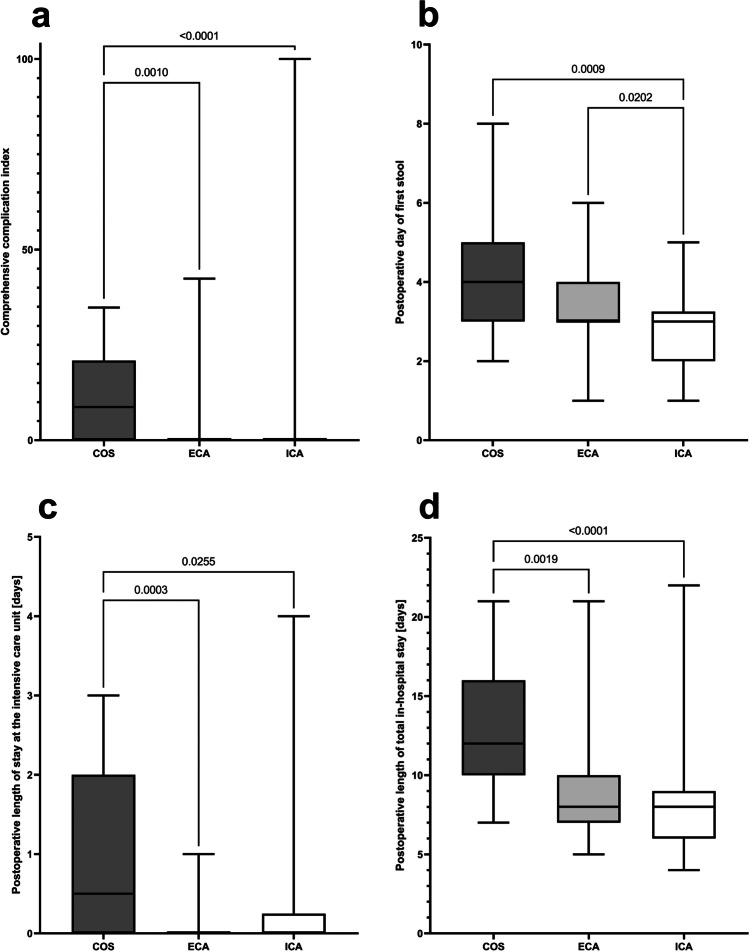
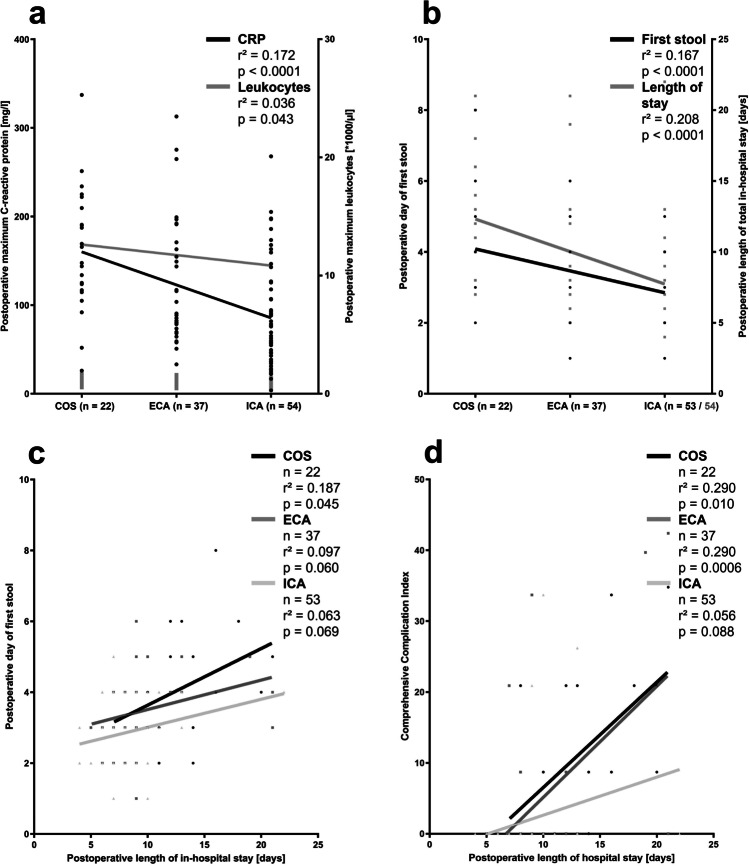
The conversion from robotic to open surgery rate was low (overall: 3.2%). Slightly longer duration of surgery had been observed during the early phase after introduction of the robotic program to RC (ECA versus COS, p = 0.044), but not anymore thereafter (versus ICA). No differences were observed in oncologic parameters including rates of tumor-negative margins, lymph node-positive patients, and lymph node yield during mesocolic excision. Both robotic approaches are beneficial regarding postoperative complication rates, especially wound infections, and shorter length of in-hospital stay compared with COS. The duration until first postoperative stool is the shortest after ICA (COS: 4 [2-8] days, ECA: 3 [1-6] days, ICA: 3 [1-5] days, p = 0.0004). Regression analyses reveal neither a longer duration of surgery nor the extent of mesocolic excision, but the degree of minimally invasiveness and postoperative systemic inflammation contribute to postoperative bowel dysfunction, which prolongs postoperative in-hospital stay significantly.
The current study reflects the institutional learning curve of oncologic RC during implementation of robotic surgery from robotic-assisted to total robotic approach without compromises in oncologic results and patient safety. However, the total robotic approach is beneficial regarding postoperative bowel recovery and general patient outcome.
右半结肠切除术(RC)是一种常见的手术。在标准传统开腹手术(COS)之下,已经引入了各种微创技术。与 COS 或传统腹腔镜相比,最近已经描述了机器人方法的几个优势。然而,新的微创技术需要与标准 COS 持续基准测试,以获得最大的患者安全性。肠功能障碍是 RC 后的常见问题。在这项研究中,术后肠恢复的一般并发症率被用作术后患者结果的替代参数。
对连续接受 COS(n=22)、机器人辅助(ECA:n=39)或全机器人手术(ICA:n=56)进行 RC 的患者进行了回顾性、10 年单中心分析。
机器人转为开腹手术的比例较低(总体:3.2%)。在引入 RC 机器人手术程序的早期,手术时间略长(ECA 与 COS 相比,p=0.044),但此后不再如此(与 ICA 相比)。在包括肿瘤阴性切缘率、淋巴结阳性患者和肠系膜切除时淋巴结产量在内的肿瘤学参数方面没有差异。两种机器人方法在术后并发症率方面均有益,特别是伤口感染和住院时间缩短与 COS 相比。第一次术后排便的时间最短的是 ICA(COS:4[2-8]天,ECA:3[1-6]天,ICA:3[1-5]天,p=0.0004)。回归分析显示,手术时间的延长或肠系膜切除的范围均与术后肠功能障碍无关,但微创程度和术后全身炎症与术后肠功能障碍有关,显著延长了术后住院时间。
本研究反映了在实施机器人手术从机器人辅助到全机器人方法的过程中,机构对 RC 肿瘤学的学习曲线,在不影响肿瘤学结果和患者安全性的情况下。然而,全机器人方法在术后肠恢复和一般患者预后方面是有益的。