University of California, San Francisco, San Francisco.
University of Rochester, Rochester, New York.
JAMA Netw Open. 2022 Jun 1;5(6):e2216370. doi: 10.1001/jamanetworkopen.2022.16370.
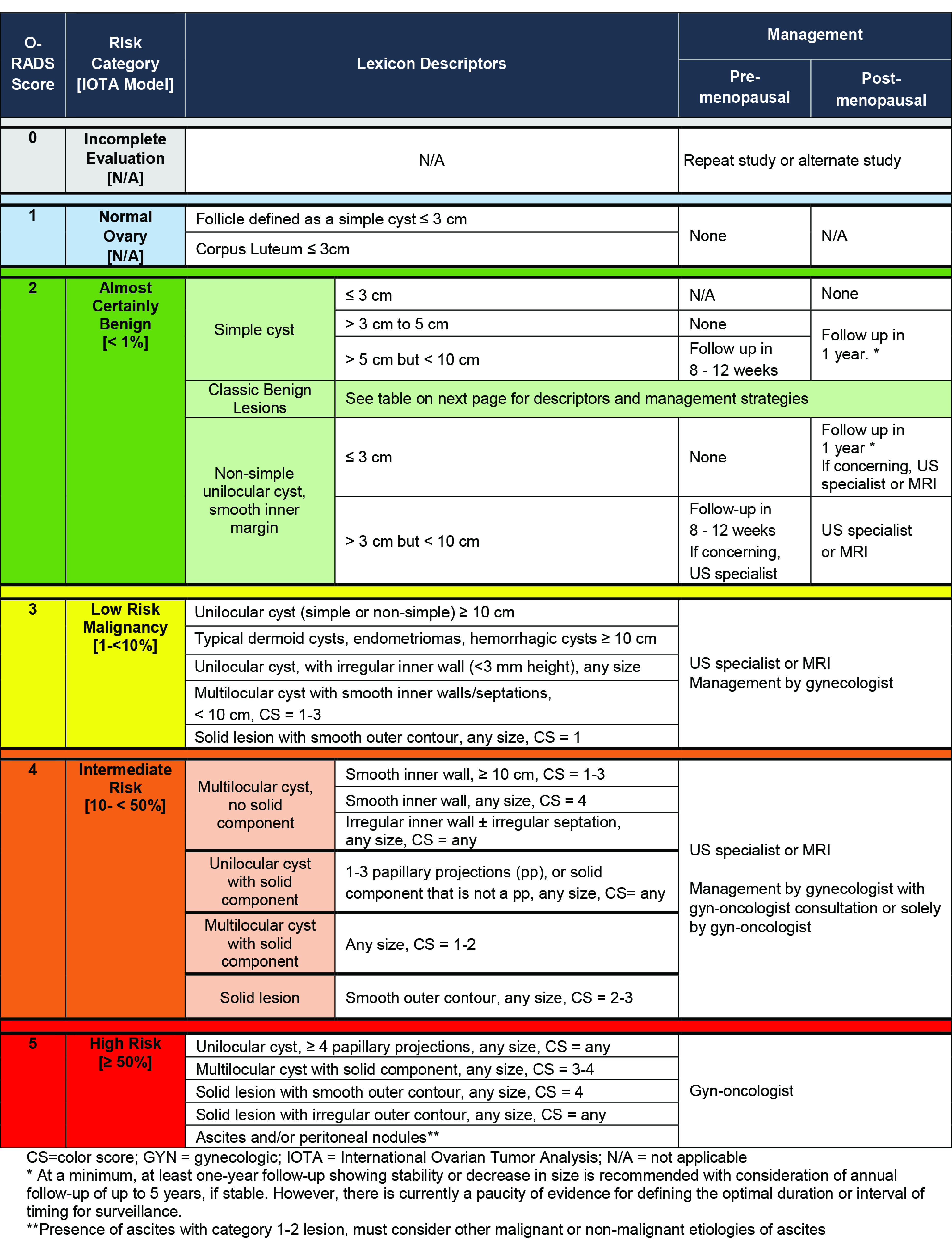
The American College of Radiology (ACR) Ovarian-Adnexal Reporting and Data System (O-RADS) ultrasound (US) risk scoring system has been studied in a selected population of women referred for suspected or known adnexal lesions. This population has a higher frequency of malignant neoplasms than women presenting to radiology departments for pelvic ultrasonography for a variety of indications, potentially impacting the diagnostic performance of the risk scoring system.
To evaluate the risk of malignant neoplasm and diagnostic performance of O-RADS US risk scoring system in a multi-institutional, nonselected cohort.
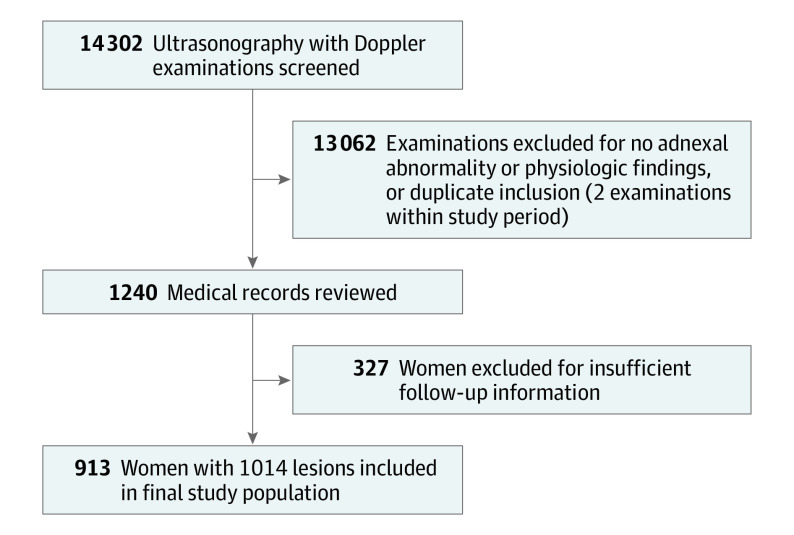
DESIGN, SETTING, AND PARTICIPANTS: This multi-institutional cohort study included a population of nonselected women in the United States who presented to radiology departments for routine pelvic ultrasonography between 2011 and 2014, with pathology confirmation imaging follow up or 2 years of clinical follow up.
Analysis of 1014 adnexal lesions using the O-RADS US risk stratification system.
Frequency of ovarian cancer and diagnostic performance of the O-RADS US risk stratification system.
This study included 913 women with 1014 adnexal lesions. The mean (SD) age of the patients was 42.4 (13.9 years), and 674 of 913 (73.8%) were premenopausal. The overall frequency of malignant neoplasm was 8.4% (85 of 1014 adnexal lesions). The frequency of malignant neoplasm for O-RADS US 2 was 0.5% (3 of 657 lesions; <1% expected); O-RADS US 3, 4.5% (5 of 112 lesions; <10% expected); O-RADS US 4, 11.6% (18 of 155; 10%-50% expected); and O-RADS 5, 65.6% (59 of 90 lesions; >50% expected). O-RADS US 4 was the optimum cutoff for diagnosing cancer with sensitivity of 90.6% (95% CI, 82.3%-95.9%), specificity of 81.9% (95% CI, 79.3%-84.3%), positive predictive value of 31.4% (95% CI, 25.7%-37.7%) and negative predictive value of 99.0% (95% CI, 98.0%-99.6%).
In this cohort study of a nonselected patient population, the O-RADS US risk stratification system performed within the expected range as published by the ACR O-RADS US committee. The frequency of malignant neoplasm was at the lower end of the published range, partially because of the lower prevalence of cancer in a nonselected population. However, a high negative predictive value was maintained, and when a lesion can be classified as an O-RADS US 2, the risk of cancer is low, which is reassuring for both clinician and patient.
美国放射学院(ACR)卵巢-附件报告和数据系统(O-RADS)超声(US)风险评分系统已在疑似或已知附件病变的特定人群中进行了研究。该人群的恶性肿瘤发病率高于因各种原因接受盆腔超声检查的放射科就诊女性,这可能会影响风险评分系统的诊断性能。
在多机构、非选择性队列中评估 O-RADS US 风险评分系统的恶性肿瘤风险和诊断性能。
设计、地点和参与者:本多机构队列研究纳入了 2011 年至 2014 年间在美国放射科就诊进行常规盆腔超声检查的非选择性女性人群,这些女性的影像学随访或临床随访时间为 2 年。
使用 O-RADS US 风险分层系统分析 1014 个附件病变。
卵巢癌的发生频率和 O-RADS US 风险分层系统的诊断性能。
本研究纳入了 913 名患有 1014 个附件病变的女性。患者的平均(SD)年龄为 42.4(13.9 岁),913 名患者中有 674 名(73.8%)处于绝经前。附件病变恶性肿瘤的总发生率为 8.4%(85/1014 个附件病变)。O-RADS US 2 的恶性肿瘤发生率为 0.5%(3/657 个病变;<1%预期);O-RADS US 3 为 4.5%(5/112 个病变;<10%预期);O-RADS US 4 为 11.6%(18/155 个病变;10%-50%预期);O-RADS 5 为 65.6%(59/90 个病变;>50%预期)。O-RADS US 4 是诊断癌症的最佳截断值,其敏感性为 90.6%(95%CI,82.3%-95.9%),特异性为 81.9%(95%CI,79.3%-84.3%),阳性预测值为 31.4%(95%CI,25.7%-37.7%),阴性预测值为 99.0%(95%CI,98.0%-99.6%)。
在这项对非选择性患者人群的队列研究中,O-RADS US 风险分层系统的表现与美国放射学院 O-RADS US 委员会公布的预期范围一致。恶性肿瘤的发生率处于公布范围的下限,部分原因是在非选择性人群中癌症的患病率较低。然而,仍保持了较高的阴性预测值,当病变可以分类为 O-RADS US 2 时,癌症的风险较低,这对临床医生和患者来说都是令人安心的。