Laboratory of Viral Diseases, National Institute of Allergy and Infectious Diseases, NIH, Bethesda, MD 20892.
Proc Natl Acad Sci U S A. 2022 Jun 14;119(24):e2202069119. doi: 10.1073/pnas.2202069119. Epub 2022 Jun 9.
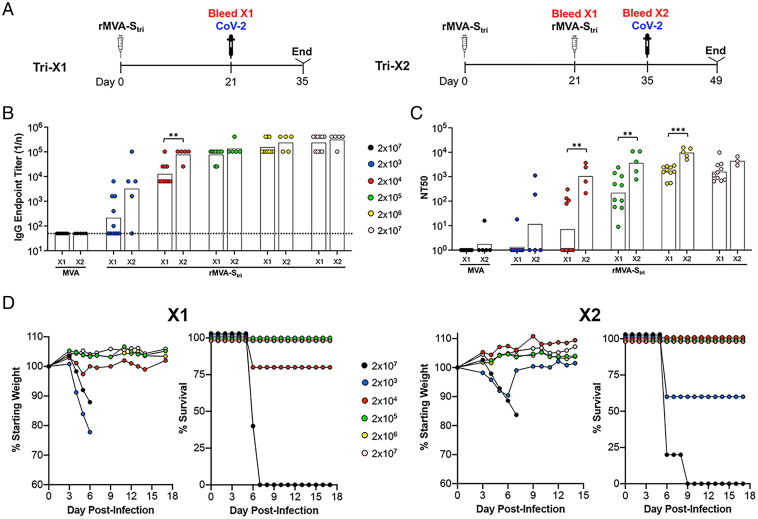
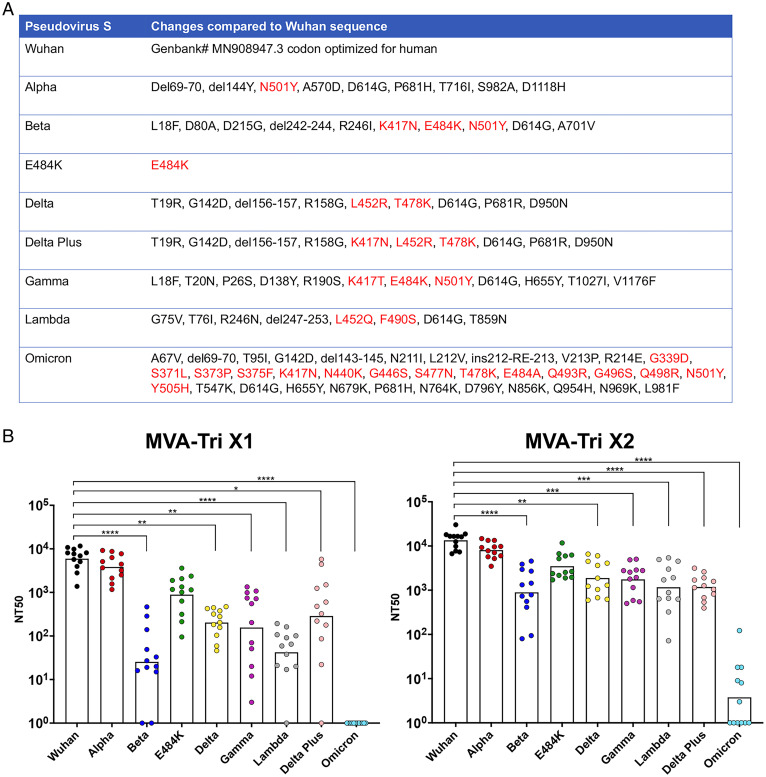
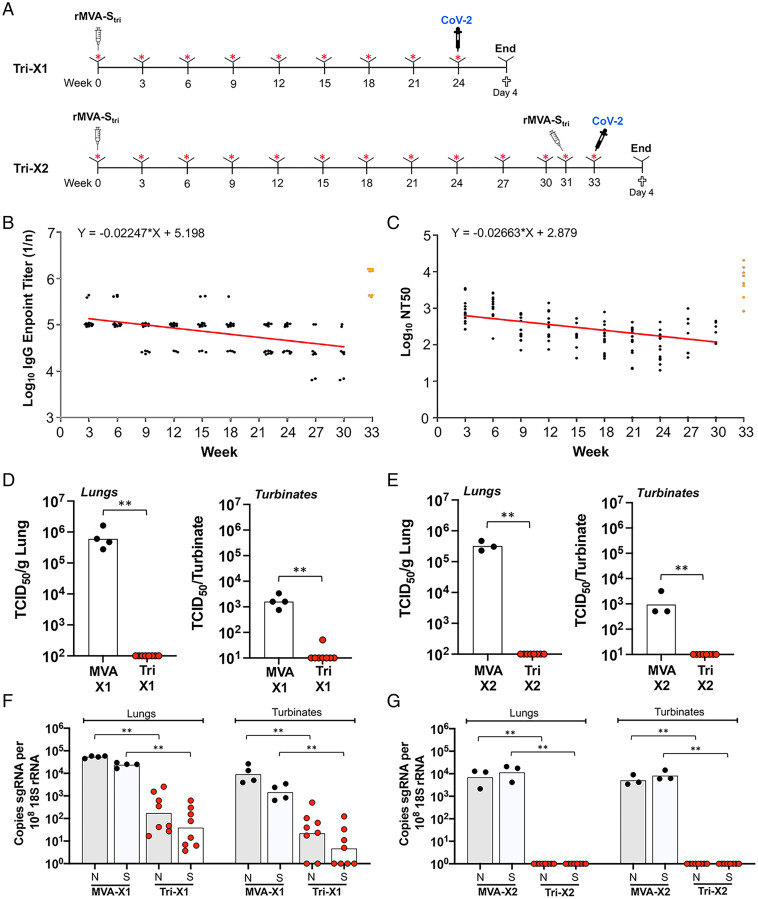
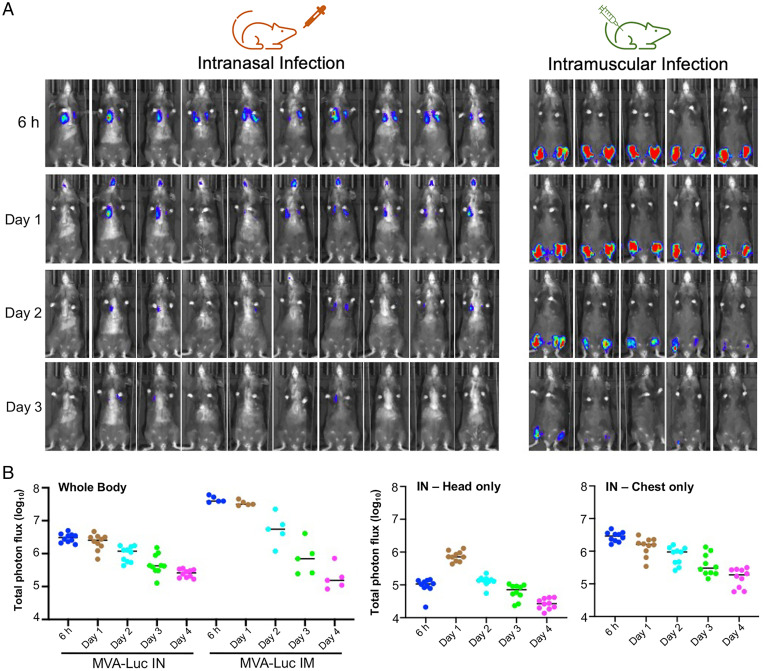
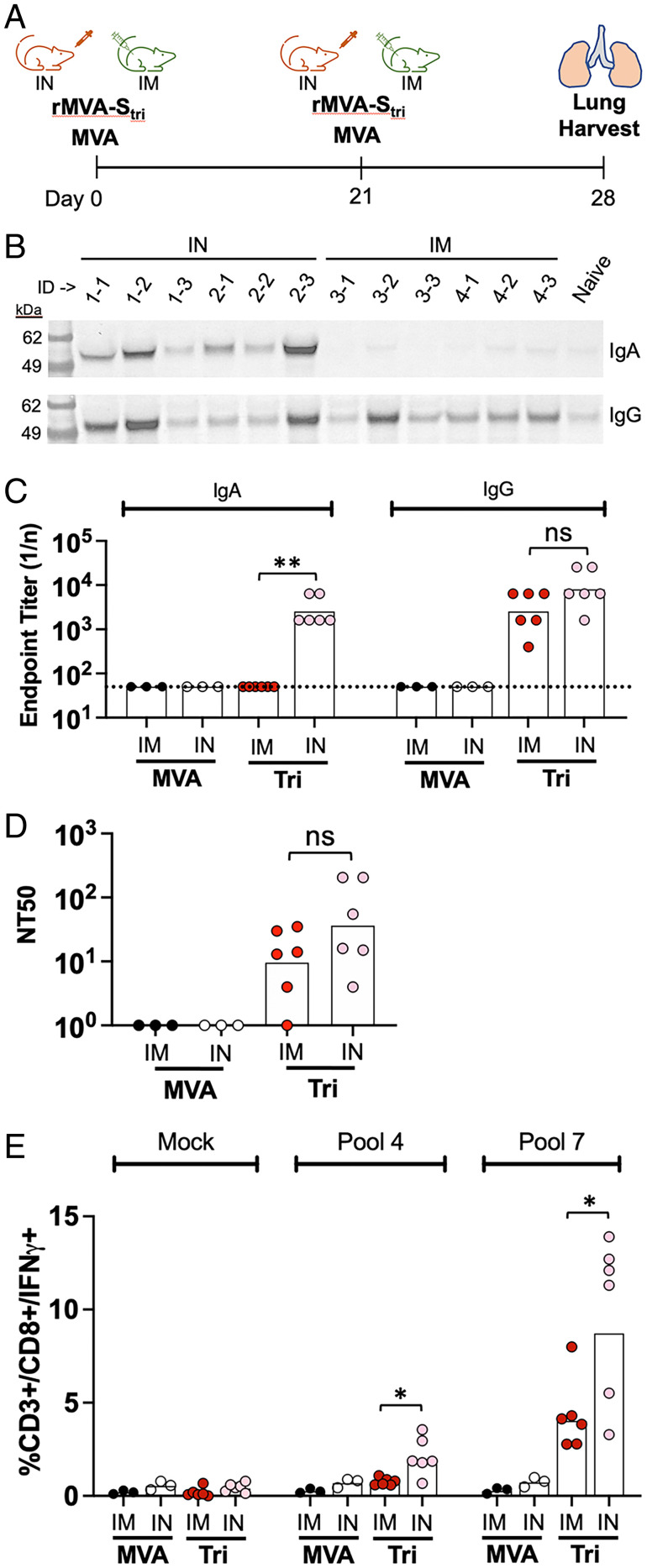
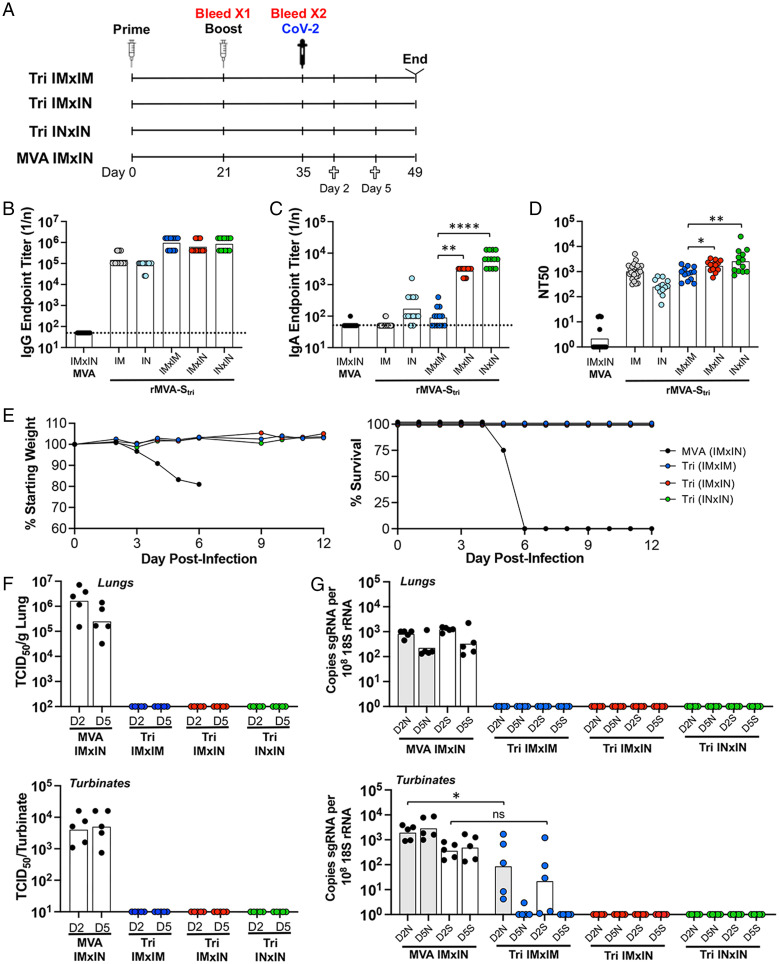
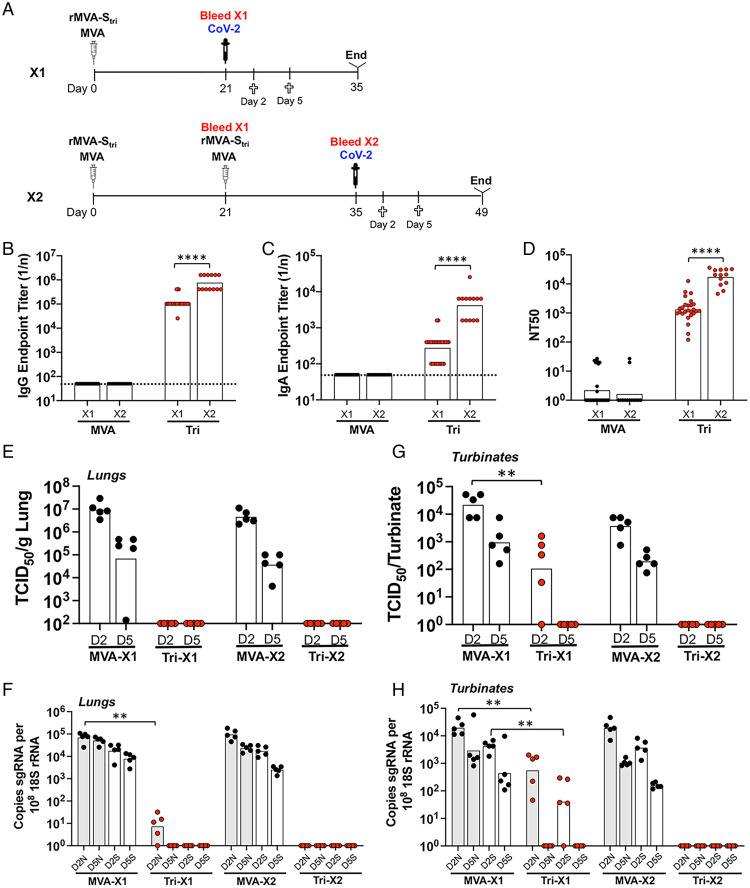
Current vaccines have greatly diminished the severity of the COVID-19 pandemic, even though they do not entirely prevent infection and transmission, likely due to insufficient immunity in the upper respiratory tract. Here, we compare intramuscular and intranasal administration of a live, replication-deficient modified vaccinia virus Ankara (MVA)-based Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) spike (S) vaccine to raise protective immune responses in the K18-hACE2 mouse model. Using a recombinant MVA expressing firefly luciferase for tracking, live imaging revealed luminescence of the respiratory tract of mice within 6 h and persisting for 3 d following intranasal inoculation, whereas luminescence remained at the site of intramuscular vaccination. Intramuscular vaccination induced S-binding-Immunoglobulin G (IgG) and neutralizing antibodies in the lungs, whereas intranasal vaccination also induced Immunoglobulin A (IgA) and higher levels of antigen-specific CD3CD8IFN-γ T cells. Similarly, IgG and neutralizing antibodies were present in the blood of mice immunized intranasally and intramuscularly, but IgA was detected only after intranasal inoculation. Intranasal boosting increased IgA after intranasal or intramuscular priming. While intramuscular vaccination prevented morbidity and cleared SARS-CoV-2 from the respiratory tract within several days after challenge, intranasal vaccination was more effective as neither infectious virus nor viral messenger (m)RNAs were detected in the nasal turbinates or lungs as early as 2 d after challenge, indicating prevention or rapid elimination of SARS-CoV-2 infection. Additionally, we determined that neutralizing antibody persisted for more than 6 mo and that serum induced to the Wuhan S protein neutralized pseudoviruses expressing the S proteins of variants, although with less potency, particularly for Beta and Omicron.
目前的疫苗大大减轻了 COVID-19 大流行的严重程度,尽管它们不能完全预防感染和传播,这可能是由于上呼吸道的免疫力不足。在这里,我们比较了肌肉内和鼻内给予活的、复制缺陷型改良痘苗病毒安卡拉(MVA)基于严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)刺突(S)疫苗,以提高 K18-hACE2 小鼠模型中的保护性免疫反应。使用表达萤火虫荧光素酶的重组 MVA 进行跟踪,活体成像显示,在鼻腔接种后 6 小时内,呼吸道发光,并持续 3 天,而肌肉内接种部位仍保持发光。肌肉内接种诱导肺部 S 结合-IgG 和中和抗体,而鼻腔接种也诱导 IgA 和更高水平的抗原特异性 CD3CD8IFN-γ T 细胞。同样,鼻腔和肌肉内免疫的小鼠血液中存在 IgG 和中和抗体,但仅在鼻腔接种后才检测到 IgA。鼻腔加强免疫可在鼻腔或肌肉内接种后增加 IgA。虽然肌肉内接种可预防发病并在挑战后数天内清除呼吸道中的 SARS-CoV-2,但鼻腔接种更为有效,因为在挑战后 2 天内,鼻甲骨或肺部均未检测到传染性病毒或病毒信使(m)RNAs,表明预防或快速消除 SARS-CoV-2 感染。此外,我们确定中和抗体持续超过 6 个月,并且针对武汉 S 蛋白的血清诱导的中和假病毒表达的 S 蛋白变体,尽管效力较低,特别是对 Beta 和 Omicron。