Institute for Physical Activity and Nutrition, Deakin University, Geelong, Victoria, Australia
Department of Public Health, Debre Markos University, Debre Markos, Amhara, Ethiopia.
Open Heart. 2022 Jun;9(1). doi: 10.1136/openhrt-2021-001949.
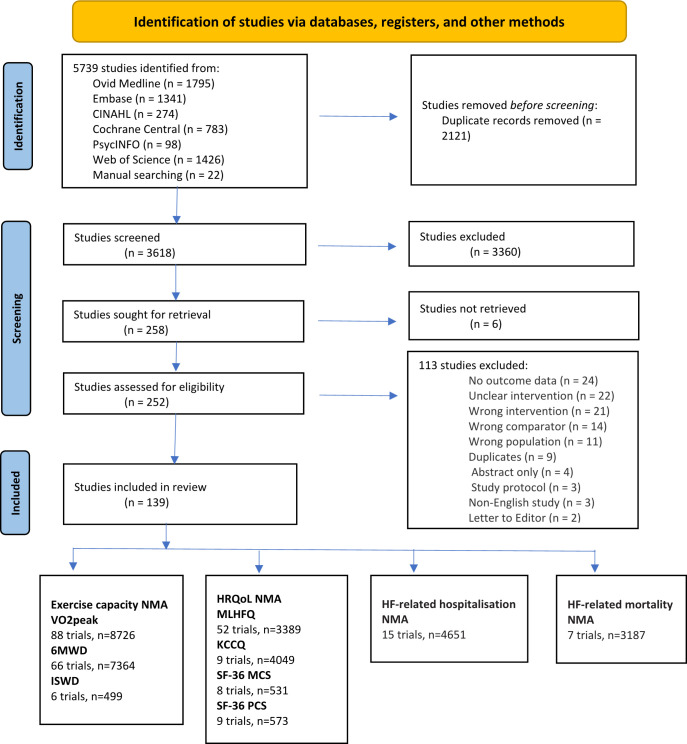
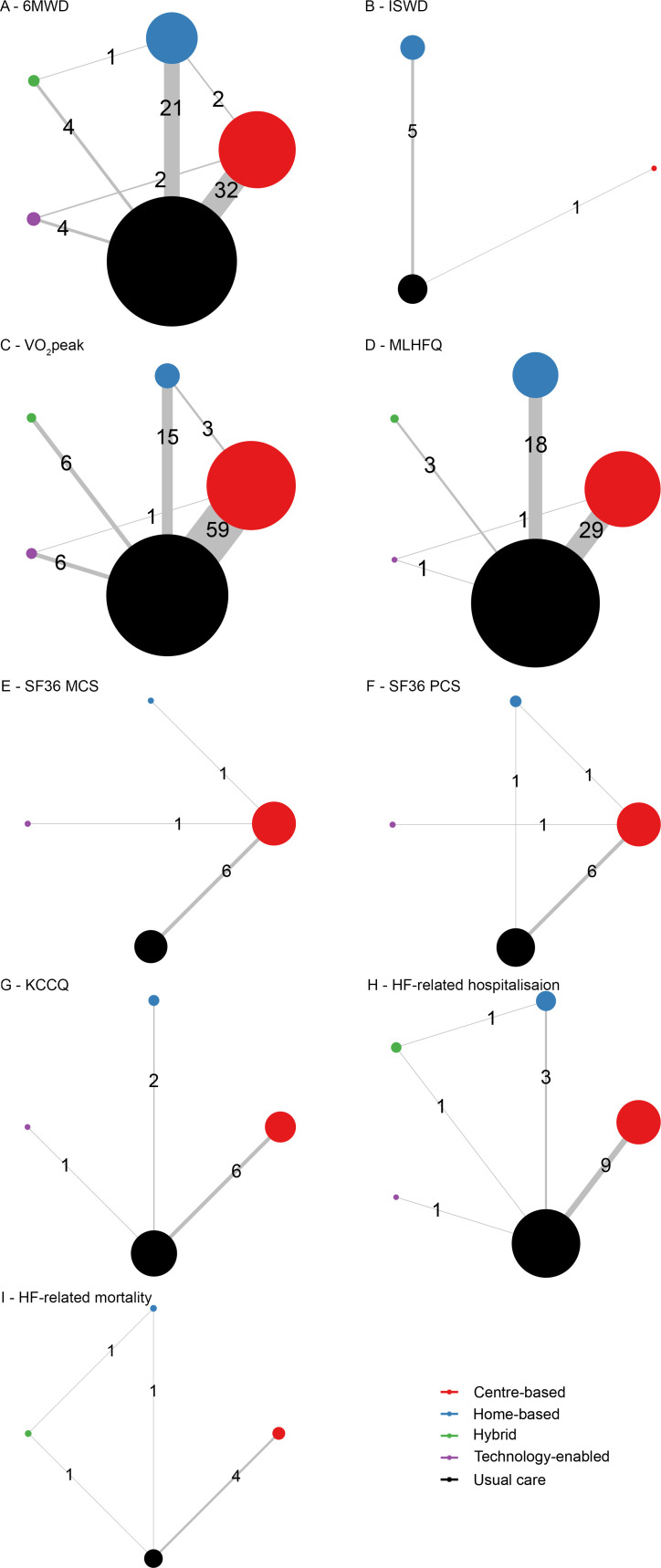
This review aimed to compare the relative effectiveness of different exercise-based cardiac rehabilitation (ExCR) delivery modes (centre-based, home-based, hybrid and technology-enabled ExCR) on key heart failure (HF) outcomes: exercise capacity, health-related quality of life (HRQoL), HF-related hospitalisation and HF-related mortality.
Randomised controlled trials (RCTs) published through 20 June 2021 were identified from six databases, and reference lists of included studies. Risk of bias and certainty of evidence were evaluated using the Cochrane tool and Grading of Recommendations Assessment, Development and Evaluation, respectively. Bayesian network meta-analysis was performed using R. Continuous and binary outcomes are reported as mean differences (MD) and ORs, respectively, with 95% credible intervals (95% CrI). One-hundred and thirty-nine RCTs (n=18 670) were included in the analysis. Network meta-analysis demonstrated improvements in VOpeak following centre-based (MD (95% CrI)=3.10 (2.56 to 3.65) mL/kg/min), home-based (MD=2.69 (1.67 to 3.70) mL/kg/min) and technology-enabled ExCR (MD=1.76 (0.27 to 3.26) mL/kg/min). Similarly, 6 min walk distance was improved following hybrid (MD=84.78 (31.64 to 138.32) m), centre-based (MD=50.35 (30.15 to 70.56) m) and home-based ExCR (MD=36.77 (12.47 to 61.29) m). Incremental shuttle walk distance did not improve following any ExCR delivery modes. Minnesota living with HF questionnaire improved after centre-based (MD=-10.38 (-14.15 to -6.46)) and home-based ExCR (MD=-8.80 (-13.62 to -4.07)). Kansas City Cardiomyopathy Questionnaire was improved following home-based ExCR (MD=20.61 (4.61 to 36.47)), and Short Form Survey 36 mental component after centre-based ExCR (MD=3.64 (0.30 to 6.14)). HF-related hospitalisation and mortality risks reduced only after centre-based ExCR (OR=0.41 (0.17 to 0.76) and OR=0.42 (0.16 to 0.90), respectively). Mean age of study participants was only associated with changes in VOpeak.
ExCR programmes have broader benefits for people with HF and since different delivery modes were comparably effective for improving exercise capacity and HRQoL, the selection of delivery modes should be tailored to individuals' preferences.
本综述旨在比较不同运动康复(ExCR)实施模式(基于中心、基于家庭、混合和技术支持的 ExCR)在关键心力衰竭(HF)结局方面的相对有效性:运动能力、健康相关生活质量(HRQoL)、HF 相关住院和 HF 相关死亡率。
通过 2021 年 6 月 20 日从六个数据库和纳入研究的参考文献列表中确定了随机对照试验(RCT)。使用 Cochrane 工具评估偏倚风险,使用 Grading of Recommendations Assessment,Development and Evaluation 评估证据确定性。使用 R 进行贝叶斯网络荟萃分析。连续和二项结果分别以均值差(MD)和比值比(OR)表示,置信区间(95%CrI)为 95%。纳入了 139 项 RCT(n=18670)进行分析。网络荟萃分析表明,中心实施的 ExCR(MD(95%CrI)=3.10(2.56 至 3.65)mL/kg/min)、家庭实施的 ExCR(MD=2.69(1.67 至 3.70)mL/kg/min)和技术支持的 ExCR(MD=1.76(0.27 至 3.26)mL/kg/min)均可改善 VOpeak。同样,混合实施的 ExCR(MD=84.78(31.64 至 138.32)m)、中心实施的 ExCR(MD=50.35(30.15 至 70.56)m)和家庭实施的 ExCR(MD=36.77(12.47 至 61.29)m)可改善 6 分钟步行距离。任何 ExCR 实施模式都不能提高增量穿梭步行距离。明尼苏达州心力衰竭生活质量问卷在中心实施的 ExCR(MD=-10.38(-14.15 至 -6.46))和家庭实施的 ExCR(MD=-8.80(-13.62 至 -4.07))后得到改善。堪萨斯城心肌病问卷在家庭实施的 ExCR 后(MD=20.61(4.61 至 36.47))和简短形式 36 心理健康成分在中心实施的 ExCR 后(MD=3.64(0.30 至 6.14))得到改善。只有中心实施的 ExCR 才能降低 HF 相关住院和死亡率风险(OR=0.41(0.17 至 0.76)和 OR=0.42(0.16 至 0.90))。研究参与者的平均年龄仅与 VOpeak 的变化相关。
ExCR 方案对心力衰竭患者有更广泛的益处,由于不同的实施模式在改善运动能力和 HRQoL 方面同样有效,因此应根据个人的喜好选择实施模式。