School of Economics and Finance, Faculty of Business and Law, Queensland University of Technology, Brisbane, Queensland, Australia; Centre for Behavioural Economics, Society and Technology, Queensland University Australia; Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Queensland, Australia.
School of Economics and Finance, Faculty of Business and Law, Queensland University of Technology, Brisbane, Queensland, Australia; Centre for Behavioural Economics, Society and Technology, Queensland University Australia; Crawford School of Public Policy, Australian National University, Canberra, Australian Capital Territory, Australia; CESifo, LMU Munich, Munich, Germany.
Gastrointest Endosc. 2022 Nov;96(5):735-742.e3. doi: 10.1016/j.gie.2022.05.023. Epub 2022 Jun 8.
Controversies exist regarding the benefits and most appropriate approach for preprocedural coronavirus disease 2019 (COVID-19) testing (eg, rapid antigen test, polymerase chain reaction, or real-time polymerase chain reaction) for outpatients undergoing diagnostic and therapeutic procedures, such as GI endoscopy, to prevent COVID-19 infections among staff. Guidelines for protecting healthcare workers (HCWs) from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection from outpatient procedures varies across medical professional organizations. This study provides an evidence-based decision support tool for key decision-makers (eg, clinicians) to respond to COVID-19 transmission risks and reduce the effect of personal biases.
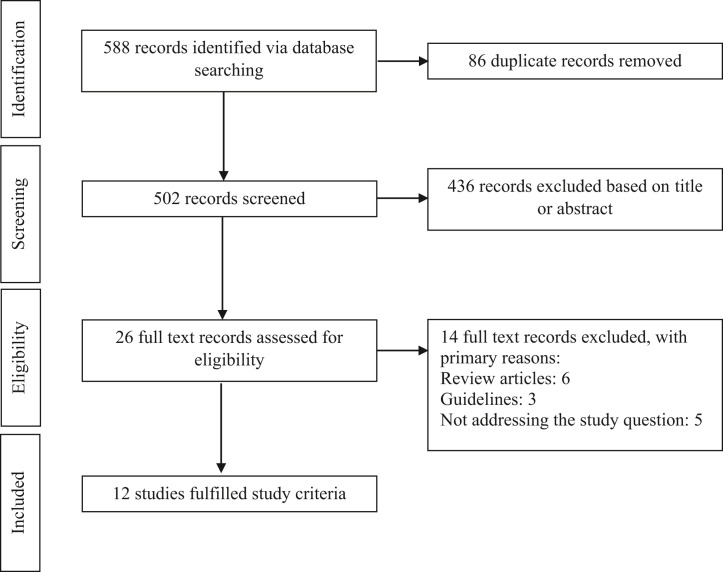
A scoping review was used to identify relevant factors influencing COVID-19 transmission risk relevant for GI endoscopy. From 12 relevant publications, 8 factors were applicable: test sensitivity, prevalence of SARS-CoV-2 in the population, age-adjusted SARS-CoV-2 prevalence in the patient cohort, proportion of asymptomatic patients, risk of transmission from asymptomatic carriers, risk reduction by personal protective equipment (PPE), vaccination rates of HCWs, and risk reduction of SAE by vaccination. The probability of a serious adverse event (SAE), such as workplace-acquired infection resulting in HCW death, under various scenarios with preprocedural testing was determined to inform decision-makers of expected costs of reductions in SAEs.
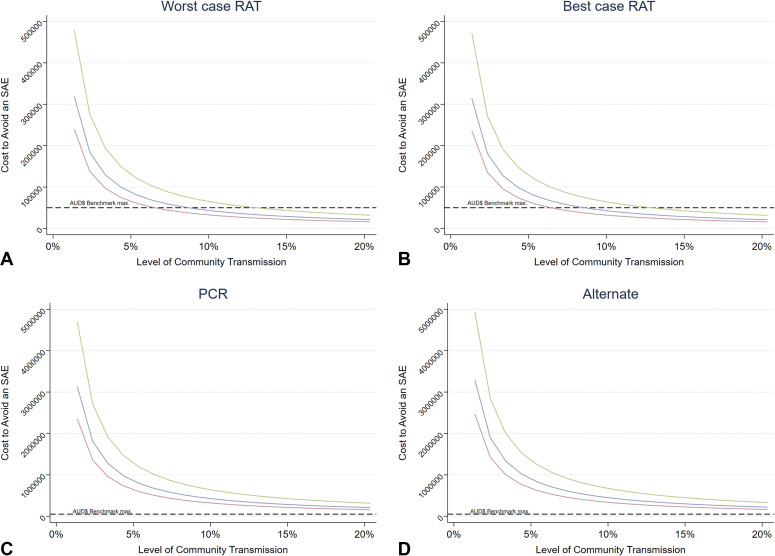
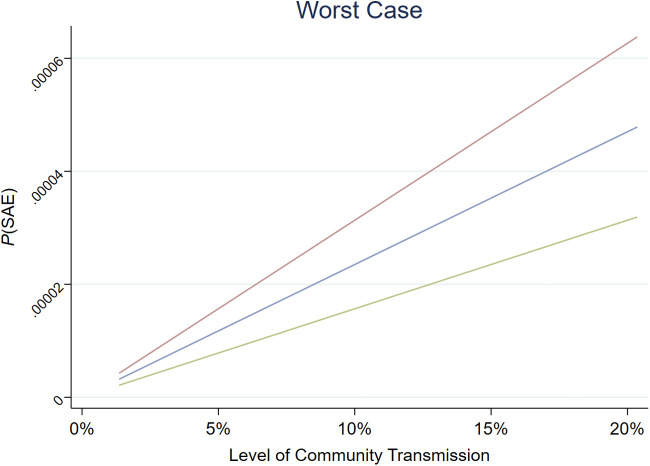
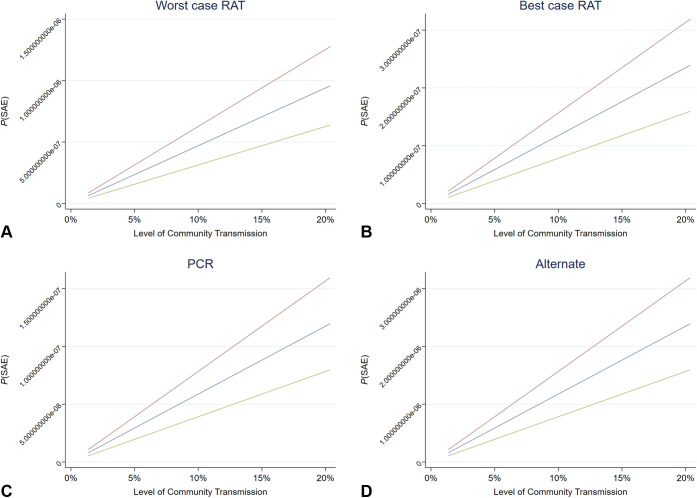
In a setting of high community transmission, without testing and PPE, 117.5 SAEs per million procedures were estimated to occur, and this was reduced to between .079 and 2.35 SAEs per million procedures with the use of PPE and preprocedural testing. When these variables are used and a range of scenarios are tested, the probability of an SAE was low even without testing but was reduced by preprocedural testing.
Under all scenarios tested, preprocedural testing reduced the SAE risk for HCWs regardless of the SARS-CoV-2 variant. Benefits of preprocedural testing are marginal when community transmission is low (eg, below 10 infections a day per 100,000 population). The proposed decision support tool can assist in developing rational preprocedural testing policies.
对于接受诊断和治疗程序(例如胃肠内镜检查)的门诊患者,进行 COVID-19(例如,快速抗原检测、聚合酶链反应或实时聚合酶链反应)的术前检测,以预防工作人员感染 COVID-19,这存在争议。保护医疗保健工作者(HCW)免受严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染的指南因医疗专业组织而异。本研究为主要决策者(例如临床医生)提供了一个基于证据的决策支持工具,以应对 COVID-19 传播风险并降低个人偏见的影响。
采用范围综述来确定与胃肠内镜相关的 COVID-19 传播风险相关的相关因素。从 12 篇相关文献中,确定了 8 个适用因素:检测灵敏度、人群中 SARS-CoV-2 的流行率、患者队列中年龄调整后的 SARS-CoV-2 流行率、无症状患者的比例、无症状携带者传播的风险、个人防护设备(PPE)降低的风险、HCW 的疫苗接种率以及疫苗接种降低 SAE 的风险。在各种术前检测情况下,确定了严重不良事件(如导致 HCW 死亡的工作场所获得性感染)的发生概率,以便决策者了解降低 SAE 的预期成本。
在社区传播率高的情况下,如果不进行检测和使用 PPE,估计每 100 万例手术会发生 117.5 例 SAE,而使用 PPE 和术前检测可将 SAE 降低至每 100 万例手术 0.079 至 2.35 例。当使用这些变量并测试各种情况时,即使不进行检测,发生 SAE 的概率也很低,但通过术前检测可以降低 SAE 的风险。
在所测试的所有情况下,术前检测均可降低 HCW 的 SAE 风险,而与 SARS-CoV-2 变体无关。当社区传播率较低(例如,每天每 10 万人中有 10 例以下感染)时,术前检测的益处微不足道。拟议的决策支持工具可以帮助制定合理的术前检测政策。