Department of Anesthesiology, Section on Critical Care Medicine, Wake Forest School of Medicine, Atrium Health Wake Forest Baptist Medical Center, Winston-Salem, NC, USA.
Outcomes Research Consortium, Cleveland, OH, USA.
J Clin Monit Comput. 2023 Feb;37(1):189-199. doi: 10.1007/s10877-022-00878-2. Epub 2022 Jun 13.
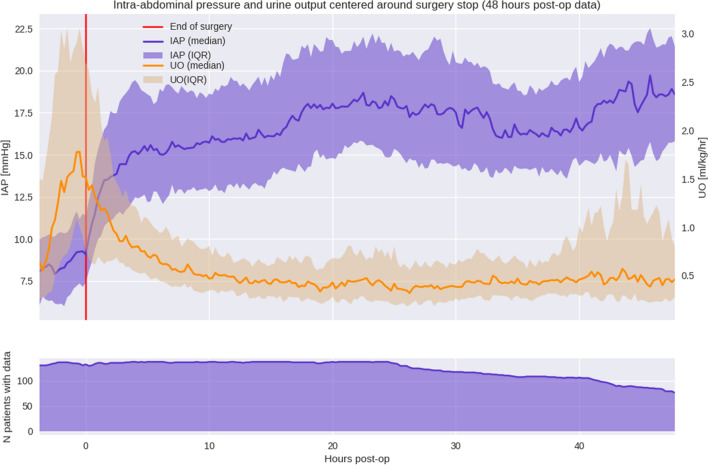
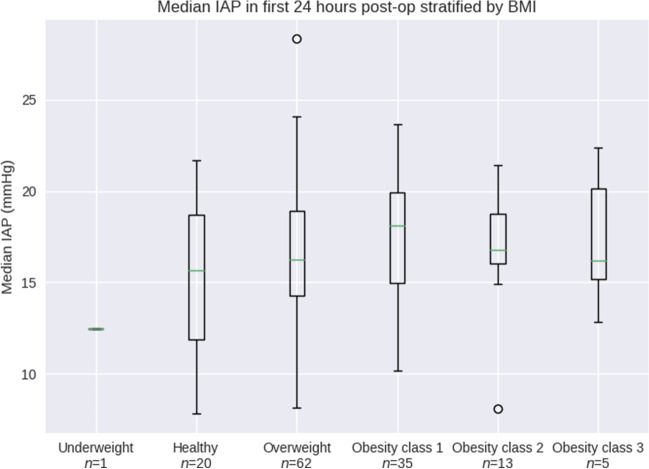
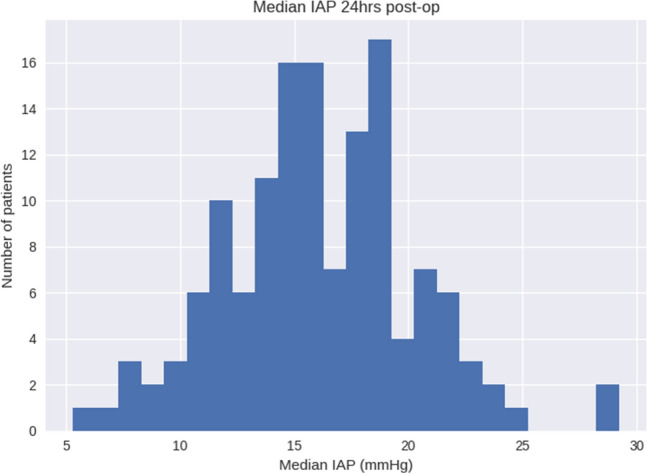
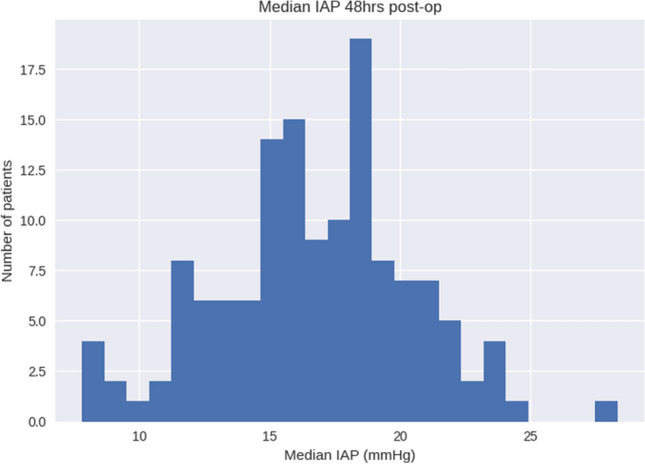
Intra-abdominal hypertension (IAH) is frequently present in the critically ill and is associated with increased morbidity and mortality. Conventionally, intermittent 'spot-check' manual measurements of bladder pressure in those perceived as high risk are used as surrogates for intra-abdominal pressure (IAP). True patterns of IAH remain unknown. We explored the incidence of IAH in cardiac surgery patients and describe the intra-and postoperative course of IAP using a novel, high frequency, automated bladder pressure measurement system. Sub-analysis of a prospective, multicenter, observational study (NCT04669548) conducted in three large academic medical centers. Continuous urinary output (CUO) and IAP measurements were observed using the Accuryn Monitoring System (Potrero Medical, Hayward, CA). Data collected included demographics, hemodynamic support, and high-frequency IAP and CUO. One Hundred Thirty-Seven cardiac surgery patients were analyzed intraoperatively and followed 48 h postoperatively in the intensive care unit. Median age was 66.4 [58.3, 72.0] years, and 61% were men. Median Foley catheter dwell time was 56.0 [46.8, 77.5] hours, and median baseline IAP was 6.3 [4.0, 8.1] mmHg. 93% (128/137) of patients were in IAH grade I, 82% (113/137) in grade II, 39% (53/137) in grade III, and 5% (7/137) in grade IV for at least 12 cumulative hours. For maximum consecutive duration of IAH, 84% (115/137) of patients spent at least 12 h in grade I, 62% (85/137) in grade II, 18% (25/137) in grade III, and 2% (3/137) in grade IV IAH. During the first 48 h after cardiac surgery, IAH is common and persistent. Improved and automated monitoring of IAP will increase the detection of IAH-which normally would remain undetected using traditional intermittent monitoring methods.
腹腔内高压(IAH)在危重病患者中很常见,与发病率和死亡率的增加有关。传统上,对被认为有高风险的患者间断地进行膀胱压力的“抽查”手动测量,作为腹腔内压力(IAP)的替代指标。IAH 的真实模式仍不清楚。我们研究了心脏手术患者中 IAH 的发生率,并使用新型高频自动膀胱压力测量系统描述了 IAP 的围手术期过程。这是一项前瞻性、多中心、观察性研究(NCT04669548)的亚分析,在三个大型学术医疗中心进行。使用 Accuryn 监测系统(Potrero Medical,Hayward,CA)观察连续尿输出量(CUO)和 IAP 测量。收集的数据包括人口统计学、血流动力学支持以及高频 IAP 和 CUO。对 137 例心脏手术患者进行了术中分析,并在重症监护病房中进行了术后 48 小时的随访。中位年龄为 66.4 [58.3,72.0] 岁,61%为男性。中位 Foley 导管留置时间为 56.0 [46.8,77.5] 小时,中位基线 IAP 为 6.3 [4.0,8.1] mmHg。93%(128/137)的患者存在 IAH Ⅰ级,82%(113/137)为Ⅱ级,39%(53/137)为Ⅲ级,5%(7/137)为Ⅳ级,至少 12 小时累积。对于 IAH 的最大连续持续时间,84%(115/137)的患者至少有 12 小时处于 IAH Ⅰ级,62%(85/137)的患者处于 IAH Ⅱ级,18%(25/137)的患者处于 IAH Ⅲ级,2%(3/137)的患者处于 IAH Ⅳ级。在心脏手术后的头 48 小时内,IAH 很常见且持续存在。对 IAP 的改进和自动化监测将增加对 IAH 的检测,而传统的间断监测方法通常会遗漏 IAH。