Hospices Civils de Lyon, Hôpital Neurologique Pierre Wertheimer, Service de Neurologie C, Centre Expert Parkinson, NS-PARK/FCRIN Network, 59 Boulevard Pinel, 69500, Bron, France.
Physiopathology of the Basal Ganglia Team, Univ Lyon, Institut des Sciences Cognitives Marc Jeannerod, CNRS, UMR 5229, 67 Boulevard Pinel, 69675, Bron, France.
Drugs Aging. 2022 Jun;39(6):417-439. doi: 10.1007/s40266-022-00942-1. Epub 2022 Jun 16.
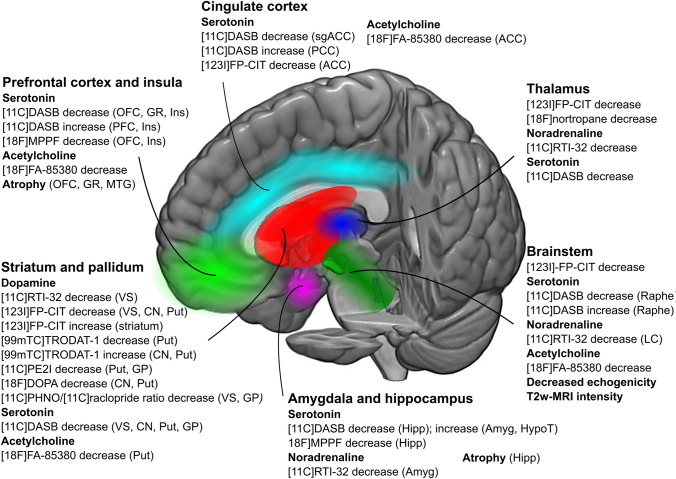
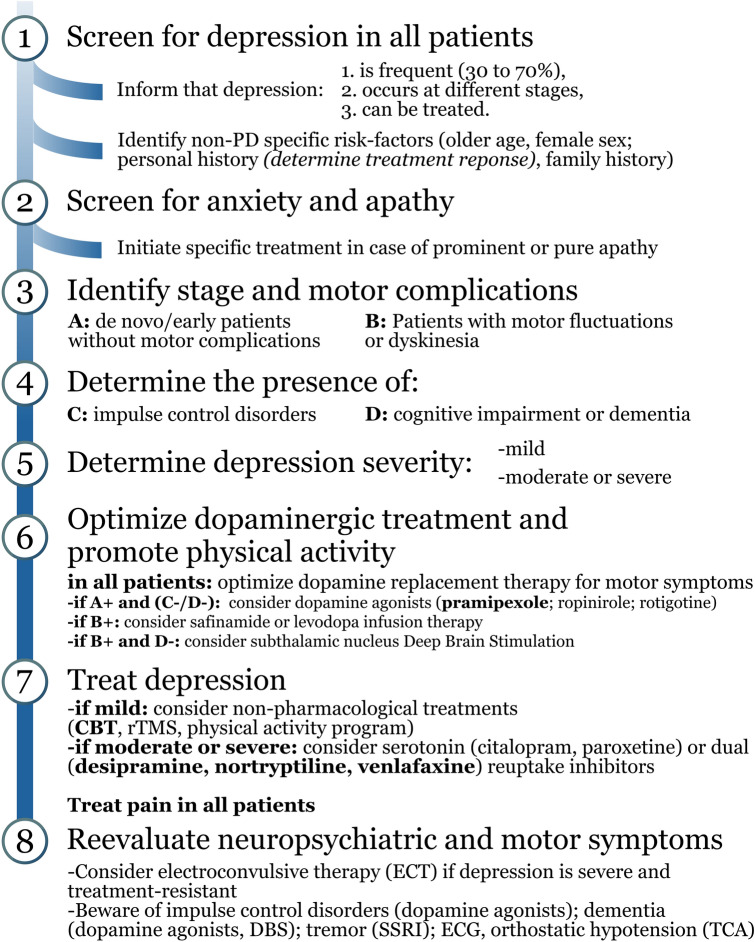
Depression is one of the most frequent and burdensome non-motor symptoms in Parkinson's disease (PD), across all stages. Even when its severity is mild, PD depression has a great impact on quality of life for these patients and their caregivers. Accordingly, accurate diagnosis, supported by validated scales, identification of risk factors, and recognition of motor and non-motor symptoms comorbid to depression are critical to understanding the neurobiology of depression, which in turn determines the effectiveness of dopaminergic drugs, antidepressants and non-pharmacological interventions. Recent advances using in vivo functional and structural imaging demonstrate that PD depression is underpinned by dysfunction of limbic networks and monoaminergic systems, depending on the stage of PD and its associated symptoms, including apathy, anxiety, rapid eye movement sleep behavior disorder (RBD), cognitive impairment and dementia. In particular, the evolution of serotonergic, noradrenergic, and dopaminergic dysfunction and abnormalities of limbic circuits across time, involving the anterior cingulate and orbitofrontal cortices, amygdala, thalamus and ventral striatum, help to delineate the variable expression of depression in patients with prodromal, early and advanced PD. Evidence is accumulating to support the use of dual serotonin and noradrenaline reuptake inhibitors (desipramine, nortriptyline, venlafaxine) in patients with PD and moderate to severe depression, while selective serotonin reuptake inhibitors, repetitive transcranial magnetic stimulation and cognitive behavioral therapy may also be considered. In all patients, recent findings advocate that optimization of dopamine replacement therapy and evaluation of deep brain stimulation of the subthalamic nucleus to improve motor symptoms represents an important first step, in addition to physical activity. Overall, this review indicates that increasing understanding of neurobiological changes help to implement a roadmap of tailored interventions for patients with PD and depression, depending on the stage and comorbid symptoms underlying PD subtypes and their prognosis.
抑郁症是帕金森病(PD)各个阶段最常见和最具负担的非运动症状之一。即使其严重程度较轻,PD 抑郁也会对这些患者及其护理人员的生活质量产生重大影响。因此,准确的诊断,支持验证的量表,识别风险因素,以及识别与抑郁共病的运动和非运动症状,对于理解抑郁的神经生物学至关重要,这反过来又决定了多巴胺能药物、抗抑郁药和非药物干预的有效性。最近使用体内功能和结构成像的进展表明,PD 抑郁是由边缘网络和单胺能系统功能障碍引起的,这取决于 PD 的阶段及其相关症状,包括冷漠、焦虑、快速眼动睡眠行为障碍(RBD)、认知障碍和痴呆症。特别是,随着时间的推移,5-羟色胺能、去甲肾上腺素能和多巴胺能功能障碍以及边缘回路的异常演变,涉及前扣带回和眶额皮质、杏仁核、丘脑和腹侧纹状体,有助于描绘前驱期、早期和晚期 PD 患者抑郁的可变表达。越来越多的证据支持在 PD 伴中度至重度抑郁的患者中使用双重 5-羟色胺和去甲肾上腺素再摄取抑制剂(地昔帕明、去甲替林、文拉法辛),而选择性 5-羟色胺再摄取抑制剂、重复经颅磁刺激和认知行为疗法也可以考虑。在所有患者中,最近的发现主张优化多巴胺替代疗法,并评估丘脑底核的深部脑刺激以改善运动症状,这是除了身体活动之外的重要第一步。总的来说,这篇综述表明,对神经生物学变化的理解的增加有助于为 PD 和抑郁患者实施个性化干预的路线图,具体取决于 PD 亚型及其预后的基础和共病症状的阶段。