Balkhy Husam H, Nisivaco Sarah, Torregrossa Gianluca, Kitahara Hiroto, Patel Brooke, Grady Kaitlin, Coleman Charocka
Department of Cardiothoracic Surgery, University of Chicago Medicine, Chicago, Ill.
JTCVS Tech. 2022 Feb 19;13:74-82. doi: 10.1016/j.xjtc.2021.12.018. eCollection 2022 Jun.
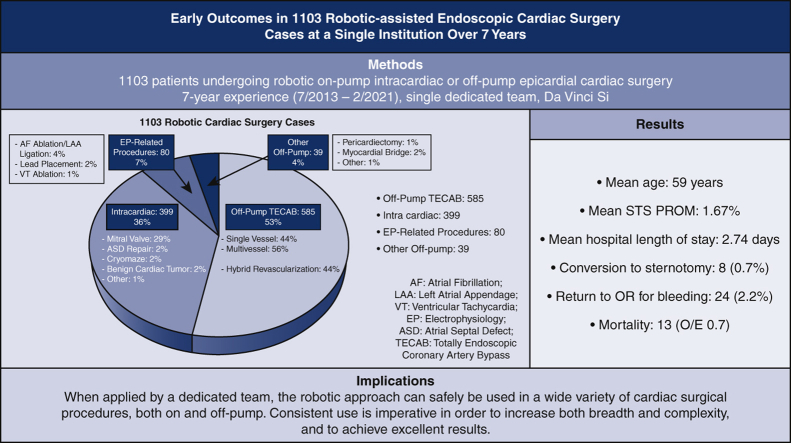
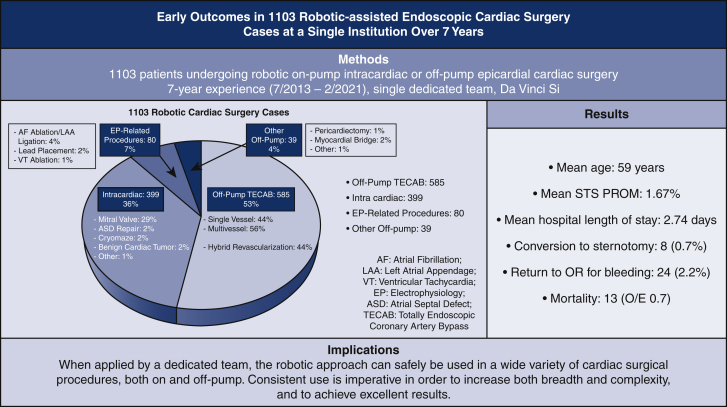
The robotic cardiac surgery program at our current institution began in 2013 with an experienced and dedicated team. This review analyzes early outcomes in the first 1103 patients.
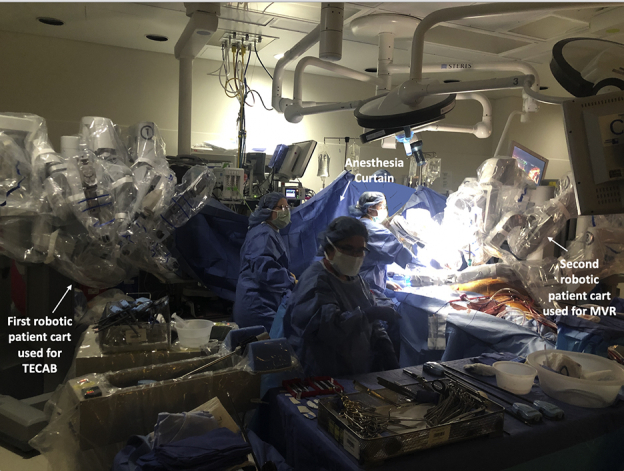
We reviewed all robotic procedures between July 2013 and February 2021. Primary outcomes were mortality and perioperative morbidity. Our robotic approach is totally endoscopic for all cases: off-pump for coronary and epicardial procedures, and on-pump with the endoballoon for mitral valve and other intracardiac procedures.
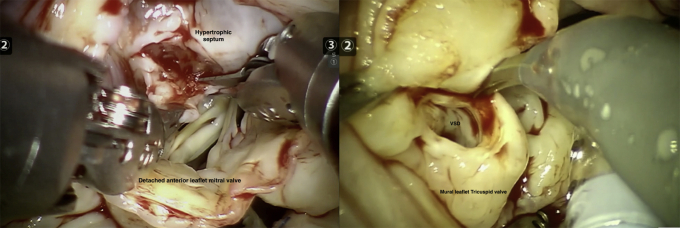
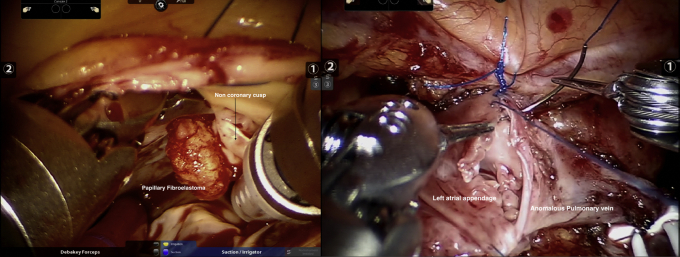
There were 1103 robotic-assisted cardiac surgeries over 7 years. A total of 585 (53%) were off-pump totally endoscopic coronary artery bypasses, 399 (36%) intracardiac cases (including isolated and concomitant mitral valve procedures, isolated tricuspid valve repair, CryoMaze, atrial or ventricular septal defect repair, benign cardiac tumor, septal myectomy, partial anomalous pulmonary venous drainage, and aortic valve replacement); 80 (7%) epicardial electrophysiology-related procedures (epicardial atrial fibrillation ablation, left atrial appendage ligation, lead placement, and ventricular tachycardia ablation); and 39 (4%) other epicardial procedures (pericardiectomy, unroofing myocardial bridge). Mortality was 1.2% (observed/expected ratio, 0.7). In the totally endoscopic coronary artery bypass and intracardiac groups, mortality was 1.0% (observed/expected, 0.6) and 1.5% (observed/expected, 0.87), respectively. There were 8 conversions to sternotomy (0.7%) and 24 (2.2%) take-backs for bleeding. Mean hospital and intensive care unit lengths of stay were 2.74 ± 1.26 days and 1.28 ± 0.57 days, respectively.
This experience demonstrates that a robotic endoscopic approach can safely be used in a multitude of cardiac surgical procedures both on- and off-pump with excellent early outcomes. An experienced surgeon and team are necessary. Longer-term follow-up is warranted.
我们当前机构的机器人心脏手术项目始于2013年,拥有一支经验丰富且专注的团队。本综述分析了前1103例患者的早期结果。
我们回顾了2013年7月至2021年2月期间的所有机器人手术。主要结果是死亡率和围手术期发病率。我们的机器人手术方法对所有病例均采用完全内镜技术:冠状动脉和心外膜手术采用非体外循环,二尖瓣和其他心内手术采用体外循环并使用心内球囊。
7年间共进行了1103例机器人辅助心脏手术。其中585例(53%)为非体外循环完全内镜冠状动脉搭桥术,399例(36%)为心内手术(包括孤立和同期二尖瓣手术、孤立三尖瓣修复、冷冻迷宫手术、房间隔或室间隔缺损修复、心脏良性肿瘤、室间隔心肌切除术、部分肺静脉异位引流和主动脉瓣置换);80例(7%)为心外膜电生理相关手术(心外膜房颤消融、左心耳结扎、导线置入和室性心动过速消融);39例(4%)为其他心外膜手术(心包切除术、心肌桥松解术)。死亡率为1.2%(观察/预期比值,0.7)。在完全内镜冠状动脉搭桥术和心内手术组中,死亡率分别为1.0%(观察/预期,0.6)和1.5%(观察/预期,0.87)。有8例转为胸骨切开术(0.7%),24例(2.2%)因出血进行了手术补救。平均住院时间和重症监护病房住院时间分别为2.74±1.26天和1.28±0.57天。
该经验表明,机器人内镜手术方法可安全用于多种心脏手术,包括体外循环和非体外循环手术,早期结果良好。需要经验丰富的外科医生和团队。有必要进行长期随访。