Niewinski Piotr, Tubek Stanislaw, Paleczny Bartlomiej, Banasiak Waldemar, Ponikowski Piotr
Institute of Heart Diseases, Wroclaw Medical University, Wroclaw, Poland.
Department of Physiology and Pathophysiology, Wroclaw Medical University, Wroclaw, Poland.
Front Physiol. 2022 May 31;13:912056. doi: 10.3389/fphys.2022.912056. eCollection 2022.
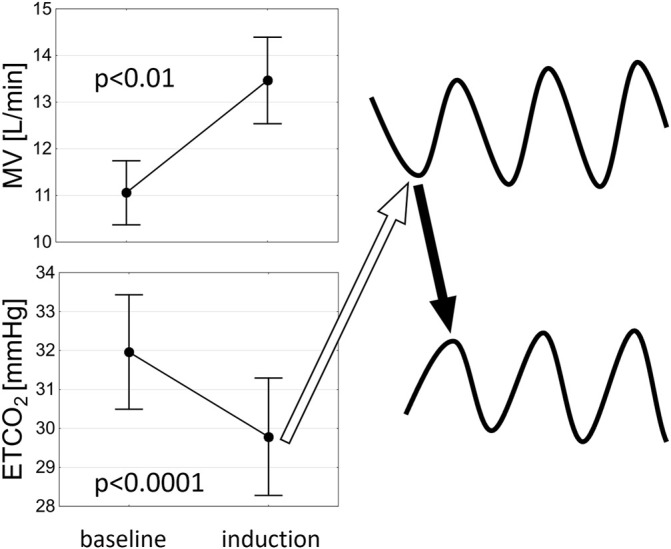
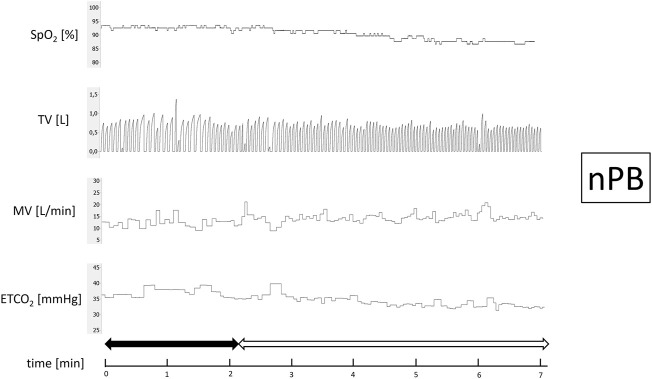
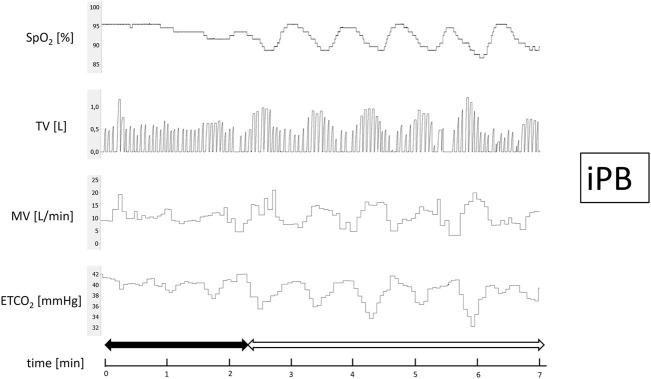
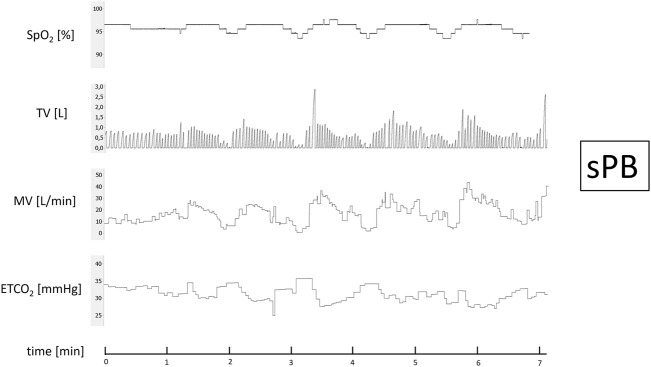
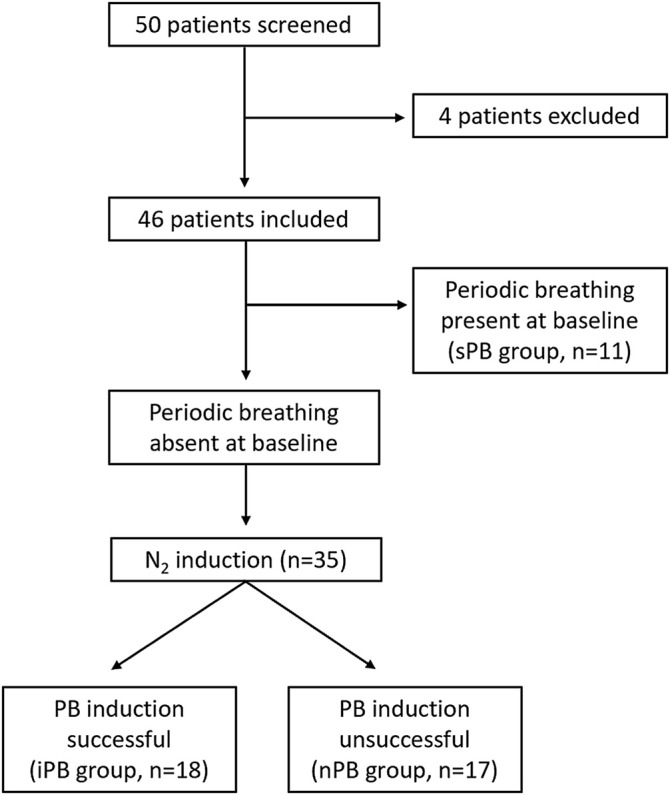
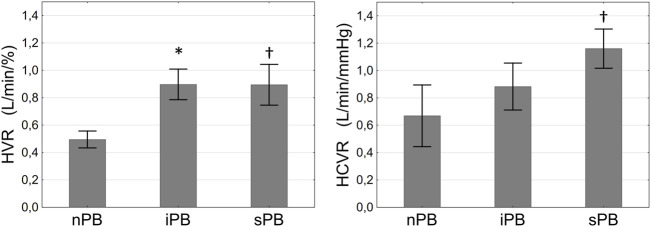
Spontaneous day-time periodic breathing (sPB) constitutes a common phenomenon in systolic heart failure (HF). However, it is unclear whether PB during wakefulness could be easily induced and what are the physiological and clinical correlates of patients with HF in whom PB induction is possible. Fifty male HF patients (age 60.8 ± 9.8 years, left ventricle ejection fraction 28.0 ± 7.4%) were prospectively screened and 46 enrolled. After exclusion of patients with sPB the remaining underwent trial of PB induction using mild hypoxia (stepwise addition of nitrogen gas to breathing mixture) which resulted in identification of inducible (iPB) in 51%. All patients underwent assessment of hypoxic ventilatory response (HVR) using transient hypoxia and of hypercapnic ventilatory response (HCVR) employing Read's rebreathing method. The induction trial did not result in any adverse events and minimal SpO during nitrogen administration was ∼85%. The iPB group (vs. non-inducible PB group, nPB) was characterized by greater HVR (0.90 ± 0.47 vs. 0.50 ± 0.26 L/min/%; <0.05) but comparable HCVR (0.88 ± 0.54 vs. 0.67 ± 0.68 L/min/mmHg; = NS) and by worse clinical and neurohormonal profile. Mean SpO which induced first cycle of PB was 88.9 ± 3.7%, while in sPB mean SpO preceding first spontaneous cycle of PB was 96.0 ± 2.5%. There was a reverse relationship between HVR and the relative variation of SpO during induced PB ( = -0.49, = 0.04). In summary, PB induction is feasible and safe in HF population using simple and standardized protocol employing incremental, mild hypoxia. Pathophysiology of iPB differs from sPB, as it relies mostly on overactive peripheral chemoreceptors. At the same time enhanced HVR might play a protective role against profound hypoxia during iPB.
自发性日间周期性呼吸(sPB)是收缩性心力衰竭(HF)中的常见现象。然而,尚不清楚清醒时的周期性呼吸是否容易诱发,以及在可能诱发周期性呼吸的HF患者中,其生理和临床关联因素是什么。前瞻性筛查了50例男性HF患者(年龄60.8±9.8岁,左心室射血分数28.0±7.4%),46例入组。排除有sPB的患者后,其余患者采用轻度低氧(向呼吸混合气中逐步添加氮气)进行周期性呼吸诱发试验,结果发现51%的患者可诱发(iPB)。所有患者均采用短暂低氧评估低氧通气反应(HVR),采用Read重复呼吸法评估高碳酸通气反应(HCVR)。诱发试验未导致任何不良事件,氮气给药期间的最低血氧饱和度(SpO)约为85%。iPB组(与不可诱发周期性呼吸组,即nPB组相比)的特点是HVR更高(0.90±0.47 vs. 0.50±0.26 L/min/%;P<0.05),但HCVR相当(0.88±0.54 vs. 0.67±0.68 L/min/mmHg;P = 无显著性差异),且临床和神经激素状况更差。诱发第一个周期性呼吸周期时的平均SpO为88.9±3.7%,而在sPB中,第一个自发性周期性呼吸周期之前的平均SpO为96.0±2.5%。在诱发的周期性呼吸期间,HVR与SpO的相对变化之间存在负相关(r = -0.49,P = 0.04)。总之,在HF人群中,使用简单标准化的递增轻度低氧方案诱发周期性呼吸是可行且安全的。iPB的病理生理学与sPB不同,因为它主要依赖外周化学感受器过度活跃。同时,增强的HVR可能在iPB期间对严重低氧起到保护作用。