Akin Muharrem, Sieweke Jan-Thorben, Garcheva Vera, Martinez Carolina Sanchez, Adel John, Plank Pia, Zandian Paris, Sühs Kurt-Wolfram, Bauersachs Johann, Schäfer Andreas
Cardiac Arrest Center, Department of Cardiology and Angiology, Hannover Medical School, Hanover, Germany.
Department of Neurology, Hannover Medical School, Hanover, Germany.
Front Cardiovasc Med. 2022 May 31;9:899583. doi: 10.3389/fcvm.2022.899583. eCollection 2022.
Patients after out-of-hospital cardiac arrest (OHCA) are at increased risk for mortality and poor neurological outcome. We assessed the additive impact of interleukin 6 (IL-6) at admission to neuron-specific enolase (NSE) at day 3 for prognosis of 30-day mortality and long-term neurological outcome in OHCA patients.
A total of 217 patients from the HAnnover COoling REgistry with return of spontaneous circulation (ROSC) after OHCA and IL-6 measurement immediately after admission during 2017-2020 were included to investigate the prognostic value and importance of IL-6 in addition to NSE obtained on day 3. Poor neurological outcome was defined by cerebral performance category (CPC) ≥ 3 after 6 months.
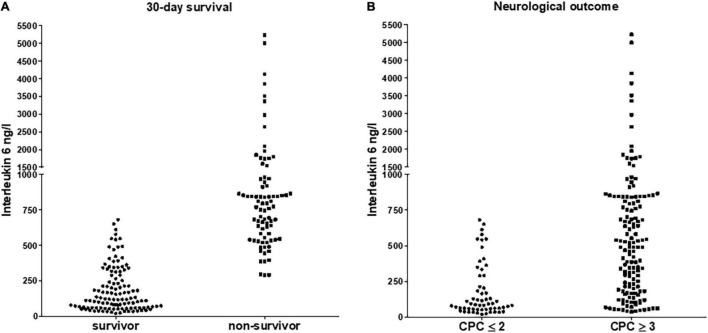
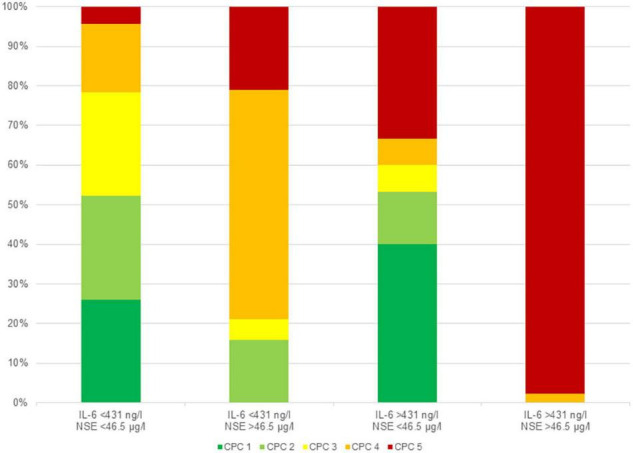
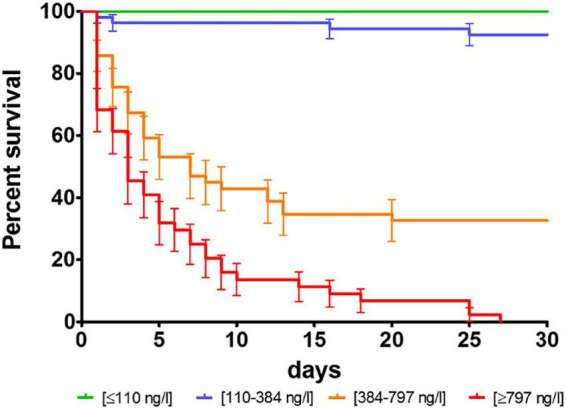
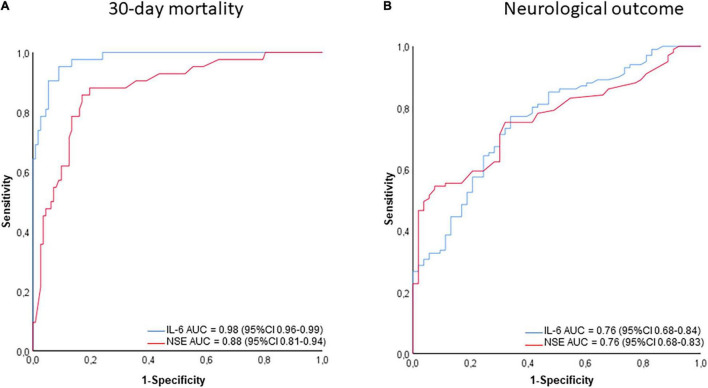
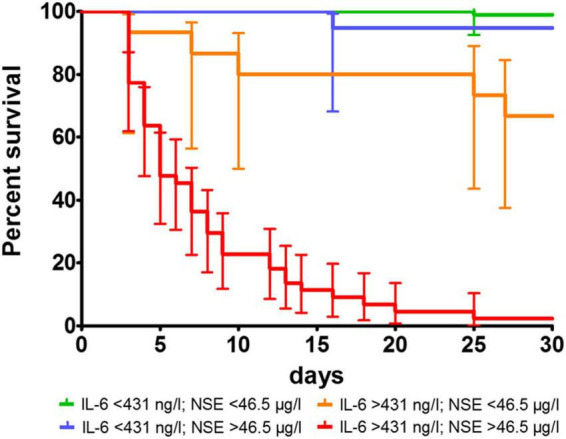
Patients with poor outcome showed higher IL-6 values (30-day mortality: 2,224 ± 524 ng/l vs 186 ± 15 ng/l, < 0.001; CPC ≥ 3 at 6 months: 1,440 ± 331 ng/l vs 180 ± 24 ng/l, < 0.001). IL-6 was an independent predictor of mortality (HR = 1.013/ng/l; 95% CI 1.007-1.019; < 0.001) and poor neurological outcome (HR = 1.004/ng/l; 95% CI 1.001-1.007; = 0.036). In ROC-analysis, AUC for IL-6 was 0.98 (95% CI 0.96-0.99) for mortality, but only 0.76 (95% CI 0.68-0.84) for poor neurological outcome. The determined cut-off value for IL-6 was 431 ng/l for mortality (NPV 89.2%). In patients with IL-6 > 431 ng/l, the combination with NSE < 46 μg/l optimally identified those individuals with potential for good neurological outcome (CPC ≤ 2).
Elevated IL-6 levels at admission after ROSC were closely associated with 30-day mortality. The combination of IL-6 and NSE provided clinically important additive information for predict poor neurological outcome at 6 months.
院外心脏骤停(OHCA)后的患者死亡风险增加,神经功能预后不良。我们评估了入院时白细胞介素6(IL-6)与第3天神经元特异性烯醇化酶(NSE)对OHCA患者30天死亡率和长期神经功能预后的附加影响。
纳入2017年至2020年期间来自汉诺威冷却登记处的217例OHCA后恢复自主循环(ROSC)且入院后立即测量IL-6的患者,以研究IL-6除第3天获得的NSE之外的预后价值和重要性。神经功能预后不良定义为6个月后脑功能分类(CPC)≥3。
预后不良的患者IL-6值更高(30天死亡率:2224±524 ng/l对186±15 ng/l,P<0.001;6个月时CPC≥3:1440±331 ng/l对180±24 ng/l,P<0.001)。IL-6是死亡率(HR = 1.013/ng/l;95%CI 1.007 - 1.019;P<0.001)和神经功能预后不良(HR = 1.004/ng/l;95%CI 1.001 - 1.007;P = 0.036)的独立预测因子。在ROC分析中,IL-6预测死亡率的AUC为0.98(95%CI 0.96 - 0.99),但预测神经功能预后不良的AUC仅为0.76(95%CI 0.68 - 0.84)。确定的IL-6死亡率临界值为431 ng/l(阴性预测值89.2%)。在IL-6>431 ng/l的患者中,与NSE<46 μg/l联合可最佳识别那些具有良好神经功能预后潜力(CPC≤2)的个体。
ROSC后入院时IL-6水平升高与30天死亡率密切相关。IL-6和NSE的联合为预测6个月时神经功能预后不良提供了重要的临床附加信息。