Yang Chao, Lan Tian, Wang Yi, Huang Wen-Hong, Li Si-Man, Li Jie, Li Feng-Ping, Li Yi-Rong, Wang Ze-Fen, Li Zhi-Qiang
Department of Neurosurgery, Zhongnan Hospital of Wuhan University, Wuhan, China.
Department of Physiology, Wuhan University School of Basic Medical Sciences, Wuhan, China.
Front Oncol. 2022 Jun 1;12:716295. doi: 10.3389/fonc.2022.716295. eCollection 2022.
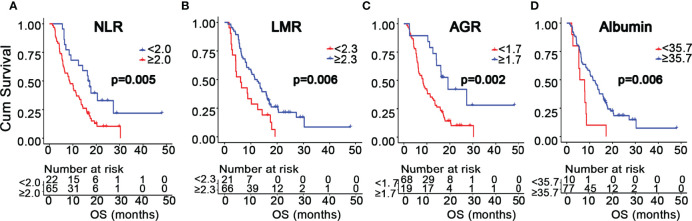
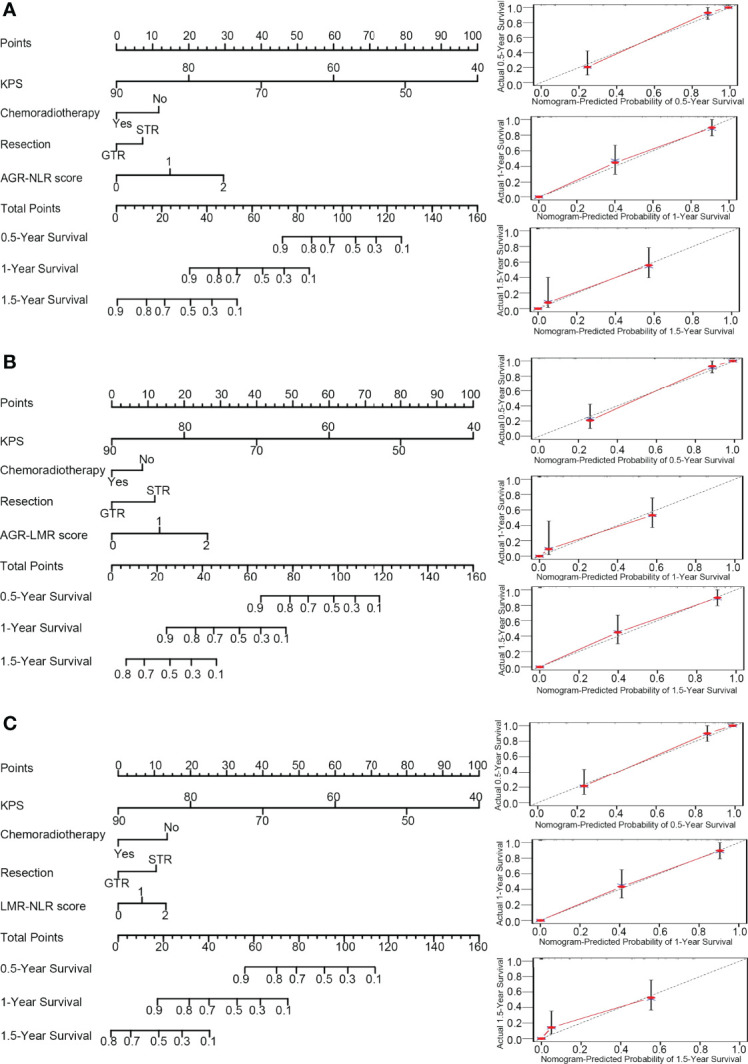
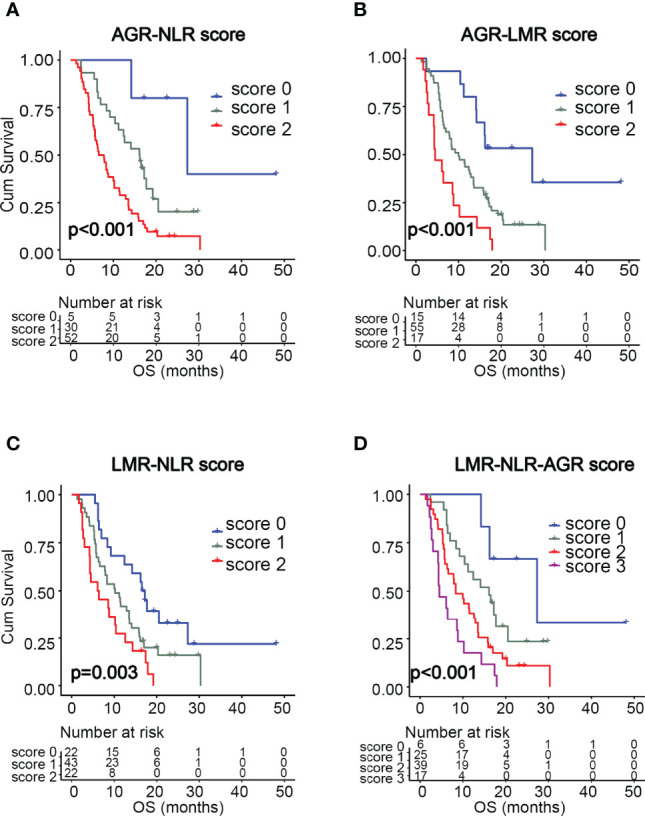
Inflammation is a hallmark of cancers. The purpose of the present study was to evaluate the prognostic potential of hematological inflammatory markers in glioblastoma multiforme (GBM) patients. The clinical data of 99 patients with lower-grade gliomas and 88 patients with GBMs were retrospectively analyzed. The optimal cutoff values for peripheral markers were determined by X-tile. Kaplan-Meier and Cox proportional hazard regression analyses were performed to identify markers with prognostic significance. Several scoring systems were constructed by combining these prognostic markers. The predictive accuracies of nomograms incorporating these scoring systems were evaluated by Harrell's concordance index and receiver operating characteristic curve analysis. GBM patients exhibited higher neutrophil counts (p=0.001), neutrophil-to-lymphocyte ratio (NLR) (p<0.001), and platelet-to-lymphocyte ratio (PLR) (p=0.001), as well as lower lymphocyte counts (p=0.023), lymphocyte-to-monocyte ratio (LMR) (p=0.015), and albumin-to-globulin ratio (AGR) (p=0.003) than those with lower-grade gliomas. Multivariate analysis indicated that a high NLR (> 2.0) (Hazard ratio[HR]=2.519, 95% confidence interval (CI): 1.220-5.204, p=0.013), low LMR (< 2.3) (HR=2.268, 95%CI: 1.172-4.386, p=0.015), or low AGR (< 1.7) (HR=2.924, 95%CI: 1.389-6.135, p=0.005) were associated with poor overall survival in GBM patients. The scoring systems of AGR-NLR, AGR-LMR, and LMR-NLR were associated with GBM survival. The nomogram integrating AGR-NLR score had the best efficacy in predicting GBM survival (c-index=0.874). Pretreatment scores of AGR-NLR, AGR-LMR, and LMR-NLR may serve as prognostic factors for GBM patients, and a nomogram integrating AGR-NLR may provide a reliable tool to facilitate personalized preoperative evaluations.
炎症是癌症的一个标志。本研究的目的是评估血液学炎症标志物在多形性胶质母细胞瘤(GBM)患者中的预后潜力。回顾性分析了99例低级别胶质瘤患者和88例GBM患者的临床资料。通过X-tile确定外周标志物的最佳临界值。进行Kaplan-Meier和Cox比例风险回归分析以识别具有预后意义的标志物。通过组合这些预后标志物构建了几种评分系统。通过Harrell一致性指数和受试者操作特征曲线分析评估纳入这些评分系统的列线图的预测准确性。与低级别胶质瘤患者相比,GBM患者的中性粒细胞计数(p = 0.001)、中性粒细胞与淋巴细胞比值(NLR)(p < 0.001)和血小板与淋巴细胞比值(PLR)(p = 0.001)更高,而淋巴细胞计数(p = 0.023)、淋巴细胞与单核细胞比值(LMR)(p = 0.015)和白蛋白与球蛋白比值(AGR)(p = 0.003)更低。多变量分析表明,高NLR(> 2.0)(风险比[HR]=2.519,95%置信区间(CI):1.220 - 5.204,p = 0.013)、低LMR(< 2.3)(HR = 2.268,95%CI:1.172 - 4.386,p = 0.015)或低AGR(< 1.7)(HR = 2.924,95%CI:1.389 - 6.135,p = 0.005)与GBM患者的总生存期较差相关。AGR - NLR、AGR - LMR和LMR - NLR的评分系统与GBM生存相关。整合AGR - NLR评分的列线图在预测GBM生存方面具有最佳疗效(c指数 = 0.874)。AGR - NLR、AGR - LMR和LMR - NLR的治疗前评分可作为GBM患者的预后因素,整合AGR - NLR的列线图可为个性化术前评估提供可靠工具。