Institute of Health Informatics, University College London, London, UK.
Department of Non-Communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK.
Kidney Int. 2022 Sep;102(3):652-660. doi: 10.1016/j.kint.2022.05.015. Epub 2022 Jun 17.
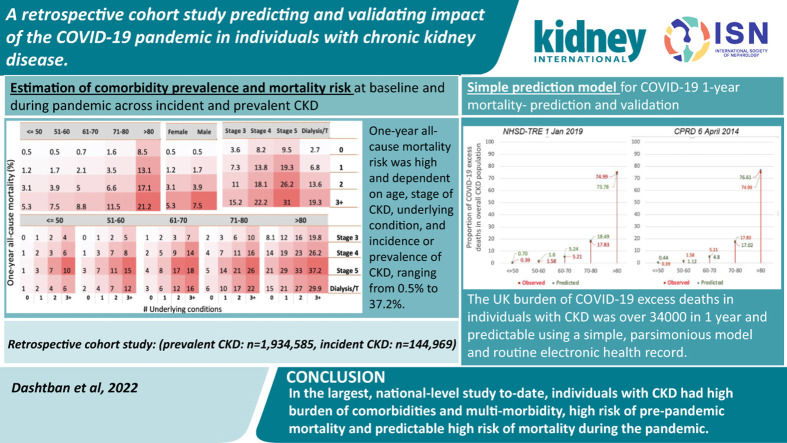
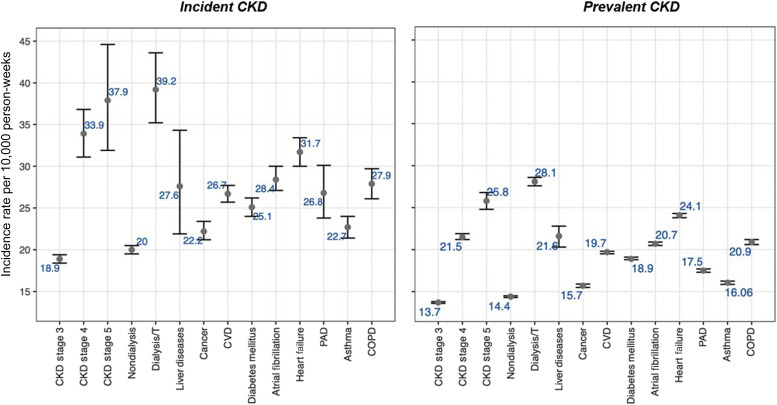
Chronic kidney disease (CKD) is associated with increased risk of baseline mortality and severe COVID-19, but analyses across CKD stages, and comorbidities are lacking. In prevalent and incident CKD, we investigated comorbidities, baseline risk, COVID-19 incidence, and predicted versus observed one-year excess death. In a national dataset (NHS Digital Trusted Research Environment [NHSD TRE]) for England encompassing 56 million individuals), we conducted a retrospective cohort study (March 2020 to March 2021) for prevalence of comorbidities by incident and prevalent CKD, SARS-CoV-2 infection and mortality. Baseline mortality risk, incidence and outcome of infection by comorbidities, controlling for age, sex and vaccination were assessed. Observed versus predicted one-year mortality at varying population infection rates and pandemic-related relative risks using our published model in pre-pandemic CKD cohorts (NHSD TRE and Clinical Practice Research Datalink [CPRD]) were compared. Among individuals with CKD (prevalent:1,934,585, incident:144,969), comorbidities were common (73.5% and 71.2% with one or more condition[s] in respective data sets, and 13.2% and 11.2% with three or more conditions, in prevalent and incident CKD), and associated with SARS-CoV-2 infection, particularly dialysis/transplantation (odds ratio 2.08, 95% confidence interval 2.04-2.13) and heart failure (1.73, 1.71-1.76), but not cancer (1.01, 1.01-1.04). One-year all-cause mortality varied by age, sex, multi-morbidity and CKD stage. Compared with 34,265 observed excess deaths, in the NHSD-TRE and CPRD databases respectively, we predicted 28,746 and 24,546 deaths (infection rates 10% and relative risks 3.0), and 23,754 and 20,283 deaths (observed infection rates 6.7% and relative risks 3.7). Thus, in this largest, national-level study, individuals with CKD have a high burden of comorbidities and multi-morbidity, and high risk of pre-pandemic and pandemic mortality. Hence, treatment of comorbidities, non-pharmaceutical measures, and vaccination are priorities for people with CKD and management of long-term conditions is important during and beyond the pandemic.
慢性肾脏病(CKD)与基线死亡率和严重 COVID-19 风险增加相关,但缺乏 CKD 各阶段和合并症的分析。在现患和新发 CKD 中,我们研究了合并症、基线风险、COVID-19 发病率以及预测与实际一年超额死亡。在英格兰的全国性数据集(NHS Digital Trusted Research Environment [NHSD TRE])中,我们对现患和新发 CKD、SARS-CoV-2 感染和死亡率中的合并症进行了回顾性队列研究(2020 年 3 月至 2021 年 3 月)。通过控制年龄、性别和疫苗接种情况,评估了合并症的基线死亡率风险、发病率和感染结局。使用我们在大流行前 CKD 队列(NHSD TRE 和临床实践研究数据链接 [CPRD])中发表的模型,比较了不同人群感染率和大流行相关相对风险下观察到的与预测的一年死亡率。
在 CKD 患者中(现患:1934585 人,新发:144969 人),合并症很常见(分别在两个数据集的一个或多个条件下占 73.5%和 71.2%,在三个或更多条件下占 13.2%和 11.2%),与 SARS-CoV-2 感染有关,特别是透析/移植(比值比 2.08,95%置信区间 2.04-2.13)和心力衰竭(1.73,1.71-1.76),但与癌症无关(1.01,1.01-1.04)。全因死亡率随年龄、性别、多合并症和 CKD 阶段而变化。与分别在 NHSD-TRE 和 CPRD 数据库中观察到的 34265 例超额死亡相比,我们预测分别有 28746 例和 24546 例死亡(感染率为 10%,相对风险为 3.0)和 23754 例和 20283 例死亡(观察到的感染率为 6.7%,相对风险为 3.7)。因此,在这项最大的国家级研究中,CKD 患者合并症和多合并症负担沉重,大流行前和大流行期间死亡率很高。因此,治疗合并症、非药物措施和疫苗接种是 CKD 患者的优先事项,长期疾病的管理在大流行期间和之后都很重要。