CIBER de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain.
Department of Pneumology, Hospital Clinic of Barcelona, Barcelona, Spain.
Intensive Care Med. 2022 Jul;48(7):850-864. doi: 10.1007/s00134-022-06726-w. Epub 2022 Jun 21.
Although there is evidence supporting the benefits of corticosteroids in patients affected with severe coronavirus disease 2019 (COVID-19), there is little information related to their potential benefits or harm in some subgroups of patients admitted to the intensive care unit (ICU) with COVID-19. We aim to investigate to find candidate variables to guide personalized treatment with steroids in critically ill patients with COVID-19.
Multicentre, observational cohort study including consecutive COVID-19 patients admitted to 55 Spanish ICUs. The primary outcome was 90-day mortality. Subsequent analyses in clinically relevant subgroups by age, ICU baseline illness severity, organ damage, laboratory findings and mechanical ventilation were performed. High doses of corticosteroids (≥ 12 mg/day equivalent dexamethasone dose), early administration of corticosteroid treatment (< 7 days since symptom onset) and long term of corticosteroids (≥ 10 days) were also investigated.
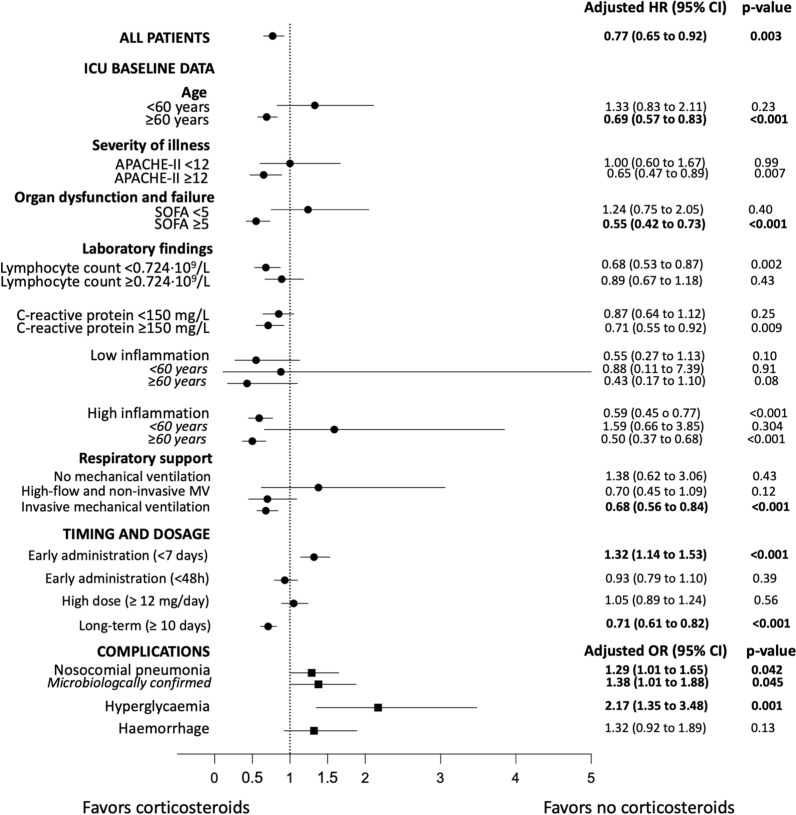
Between February 2020 and October 2021, 4226 patients were included. Of these, 3592 (85%) patients had received systemic corticosteroids during hospitalisation. In the propensity-adjusted multivariable analysis, the use of corticosteroids was protective for 90-day mortality in the overall population (HR 0.77 [0.65-0.92], p = 0.003) and in-hospital mortality (SHR 0.70 [0.58-0.84], p < 0.001). Significant effect modification was found after adjustment for covariates using propensity score for age (p = 0.001 interaction term), Sequential Organ Failure Assessment (SOFA) score (p = 0.014 interaction term), and mechanical ventilation (p = 0.001 interaction term). We observed a beneficial effect of corticosteroids on 90-day mortality in various patient subgroups, including those patients aged ≥ 60 years; those with higher baseline severity; and those receiving invasive mechanical ventilation at ICU admission. Early administration was associated with a higher risk of 90-day mortality in the overall population (HR 1.32 [1.14-1.53], p < 0.001). Long-term use was associated with a lower risk of 90-day mortality in the overall population (HR 0.71 [0.61-0.82], p < 0.001). No effect was found regarding the dosage of corticosteroids. Moreover, the use of corticosteroids was associated with an increased risk of nosocomial bacterial pneumonia and hyperglycaemia.
Corticosteroid in ICU-admitted patients with COVID-19 may be administered based on age, severity, baseline inflammation, and invasive mechanical ventilation. Early administration since symptom onset may prove harmful.
虽然有证据支持皮质类固醇在重症 2019 年冠状病毒病(COVID-19)患者中的益处,但在因 COVID-19 入住重症监护病房(ICU)的某些亚组患者中,有关皮质类固醇潜在益处或危害的信息却很少。我们旨在调查候选变量,以指导危重症 COVID-19 患者的皮质类固醇个体化治疗。
这是一项多中心、观察性队列研究,纳入了西班牙 55 家 ICU 连续收治的 COVID-19 患者。主要结局为 90 天死亡率。随后在年龄、ICU 基线疾病严重程度、器官损伤、实验室发现和机械通气等临床相关亚组中进行了分析。还研究了高剂量皮质类固醇(≥12mg/天等效地塞米松剂量)、皮质类固醇治疗早期给药(症状出现后<7 天)和皮质类固醇长期应用(≥10 天)。
2020 年 2 月至 2021 年 10 月期间,共纳入 4226 例患者。其中,3592 例(85%)患者在住院期间接受了全身皮质类固醇治疗。在倾向评分调整的多变量分析中,皮质类固醇的使用对全人群(HR 0.77 [0.65-0.92],p=0.003)和院内死亡率(SHR 0.70 [0.58-0.84],p<0.001)均有保护作用。在使用倾向评分调整年龄(p=0.001 交互项)、序贯器官衰竭评估(SOFA)评分(p=0.014 交互项)和机械通气(p=0.001 交互项)进行协变量调整后,发现了显著的效应修饰。我们观察到皮质类固醇在包括≥60 岁患者;基线严重程度较高的患者;以及在 ICU 入院时接受有创机械通气的患者在内的各种患者亚组中对 90 天死亡率均有有益影响。皮质类固醇的早期给药与全人群 90 天死亡率升高相关(HR 1.32 [1.14-1.53],p<0.001)。皮质类固醇长期应用与全人群 90 天死亡率降低相关(HR 0.71 [0.61-0.82],p<0.001)。皮质类固醇的剂量没有效果。此外,皮质类固醇的使用与医院获得性细菌性肺炎和高血糖的风险增加有关。
对于因 COVID-19 入住 ICU 的患者,可以根据年龄、严重程度、基线炎症和有创机械通气来使用皮质类固醇。从症状出现开始的早期给药可能有害。