Centre for Safe Medication Practice and Research, Department of Pharmacology and Pharmacy, General Office, L02-56 2/F, Laboratory Block, LKS Faculty of Medicine, The University of Hong Kong, 21 Sassoon Road, Pokfulam, Hong Kong SAR, China.
Laboratory of Data Discovery for Health (D24H), Hong Kong SAR, China.
Cardiovasc Res. 2022 Jul 27;118(10):2329-2338. doi: 10.1093/cvr/cvac068.
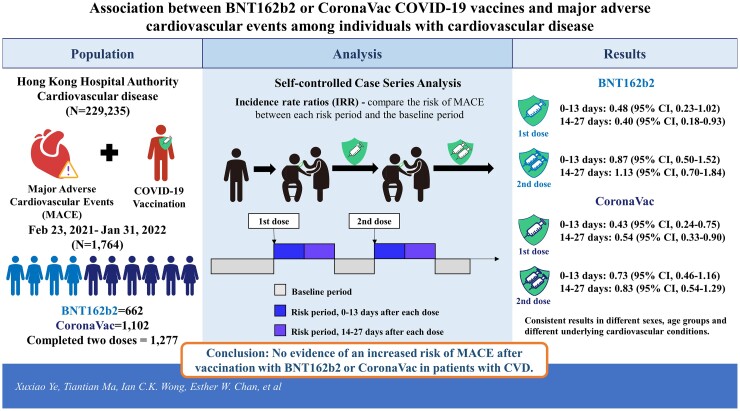
Concern about the cardiovascular safety of coronavirus disease 2019 (COVID-19) vaccines among individuals with cardiovascular disease (CVD) may lead to vaccine hesitancy. We sought to assess the association between two COVID-19 vaccines, BNT162b2 and CoronaVac, and the risk of major adverse cardiovascular events (MACE) in individuals with established CVD.
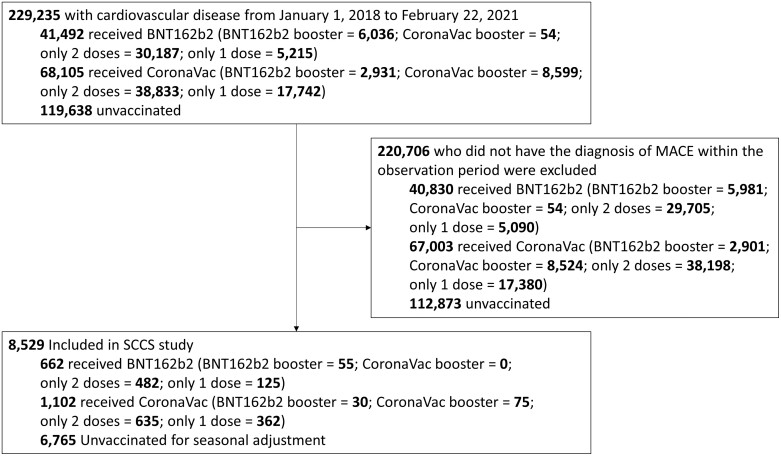
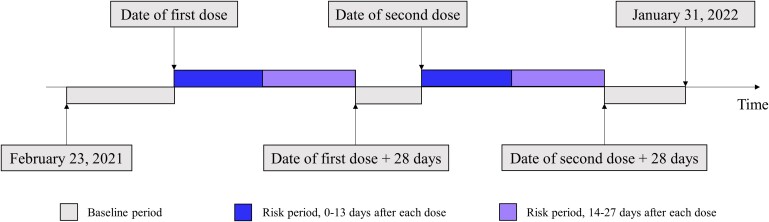
We identified individuals with a history of CVD before 23 February 2021 and a diagnosis of MACE between 23 February 2021 and 31 January 2022 in Hong Kong. MACE was defined as a composite of myocardial infarction, stroke, revascularization, and cardiovascular death. Electronic health records from the Hong Kong Hospital Authority were linked to vaccination records from the Department of Health. A self-controlled case-series method was used to evaluate the risk of MACE for 0-13 and 14-27 days after two doses of COVID-19 vaccine. We estimated incidence rate ratios (IRRs) to compare the risk of MACE between each risk period and the baseline period. A total of 229 235 individuals with CVD were identified, of which 1764 were vaccinated and had a diagnosis of MACE during the observation period (BNT162b2 = 662; CoronaVac = 1102). For BNT162b2, IRRs were 0.48 [95% confidence interval (CI) 0.23-1.02] for the first dose and 0.87 (95% CI 0.50-1.52) for the second dose during the 0-13 days risk period, 0.40 (95% CI 0.18-0.93) for the first dose and 1.13 (95% CI 0.70-1.84) for the second dose during the 14-27 days risk period. For CoronaVac, the IRRs were 0.43 (95% CI 0.24-0.75) for the first dose and, 0.73 (95% CI 0.46-1.16) for the second dose during the 0-13 days risk period, 0.54 (95% CI 0.33-0.90) for the first dose and 0.83 (95% CI 0.54-1.29) for the second dose during the 14-27 days risk period. Consistent results were found in subgroup analyses for different sexes, age groups and different underlying cardiovascular conditions.
Our findings showed no evidence of an increased risk of MACE after vaccination with BNT162b2 or CoronaVac in patients with CVD. Future research is required to monitor the risk after the third dose of each vaccine.
在心血管疾病(CVD)患者中,对 2019 年冠状病毒病(COVID-19)疫苗的心血管安全性的担忧可能导致疫苗犹豫。我们旨在评估两种 COVID-19 疫苗,BNT162b2 和科兴疫苗,与已确诊 CVD 患者的主要不良心血管事件(MACE)风险之间的关联。
我们在香港确定了 2021 年 2 月 23 日之前有 CVD 病史且在 2021 年 2 月 23 日至 2022 年 1 月 31 日之间诊断为 MACE 的患者。MACE 定义为心肌梗死、中风、血运重建和心血管死亡的综合指标。将香港医院管理局的电子健康记录与卫生署的疫苗接种记录相链接。采用自对照病例系列方法评估 COVID-19 疫苗两剂后 0-13 天和 14-27 天内 MACE 的风险。我们估计发病率比值(IRR)以比较每个风险期与基线期之间的 MACE 风险。共确定了 229235 例 CVD 患者,其中 1764 例接受了疫苗接种,并在观察期内诊断出 MACE(BNT162b2=662;科兴=1102)。对于 BNT162b2,第一剂的 IRR 为 0.48(95%置信区间 0.23-1.02),第二剂为 0.87(95%置信区间 0.50-1.52)在 0-13 天风险期内,第一剂的 IRR 为 0.40(95%置信区间 0.18-0.93),第二剂的 IRR 为 1.13(95%置信区间 0.70-1.84)在 14-27 天风险期内。对于科兴疫苗,第一剂的 IRR 为 0.43(95%置信区间 0.24-0.75),第二剂的 IRR 为 0.73(95%置信区间 0.46-1.16)在 0-13 天风险期内,第一剂的 IRR 为 0.54(95%置信区间 0.33-0.90),第二剂的 IRR 为 0.83(95%置信区间 0.54-1.29)在 14-27 天风险期内。在不同性别、年龄组和不同基础心血管疾病的亚组分析中,均得到了一致的结果。
我们的研究结果表明,在 CVD 患者中接种 BNT162b2 或科兴疫苗后,MACE 风险没有增加的证据。需要进一步研究以监测每种疫苗第三剂后的风险。