Böcker Arne, Aman Martin, Kneser Ulrich, Harhaus Leila, Siemers Frank, Stang Felix
Department of Hand-, Plastic and Reconstructive Surgery, Burn Center, Department of Plastic and Hand Surgery, University of Heidelberg, BG Trauma Hospital Ludwigshafen, 67071 Ludwigshafen, Germany.
Department of Plastic- and Hand Surgery, Burn Center, Martin-Luther University Halle-Wittenberg, BG Trauma Center Bermannstrost, 06002 Halle, Germany.
J Pers Med. 2022 May 30;12(6):900. doi: 10.3390/jpm12060900.
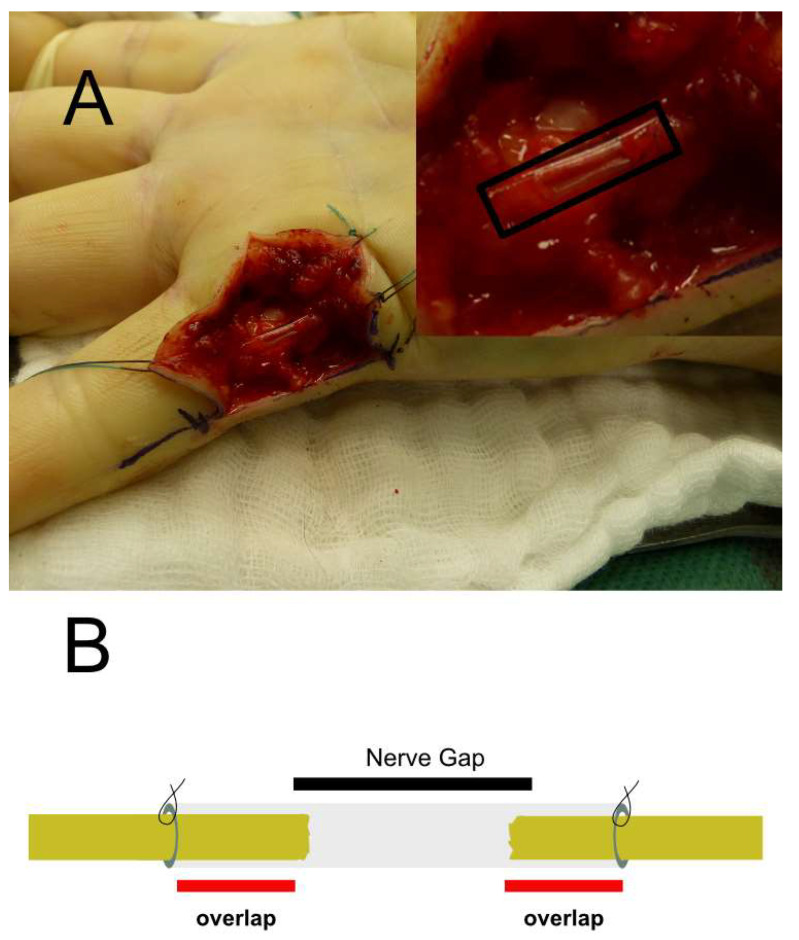
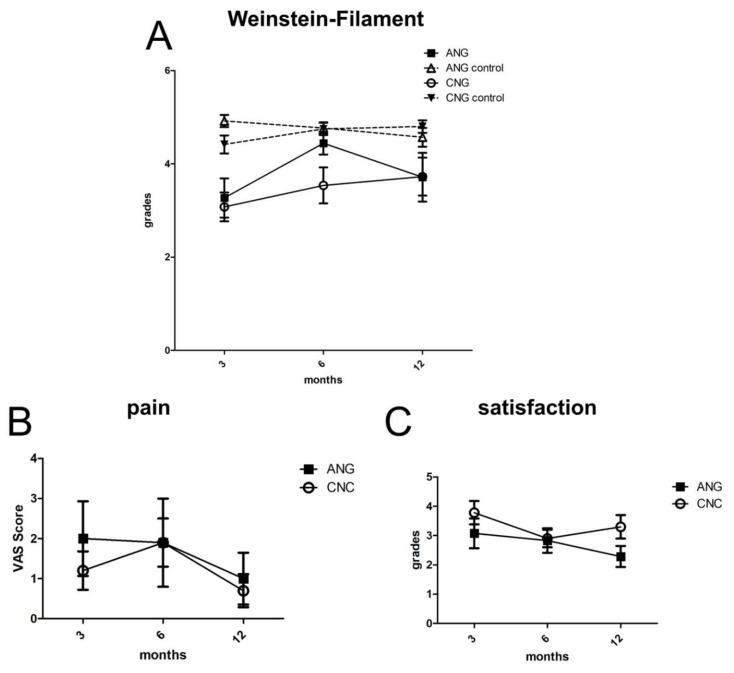
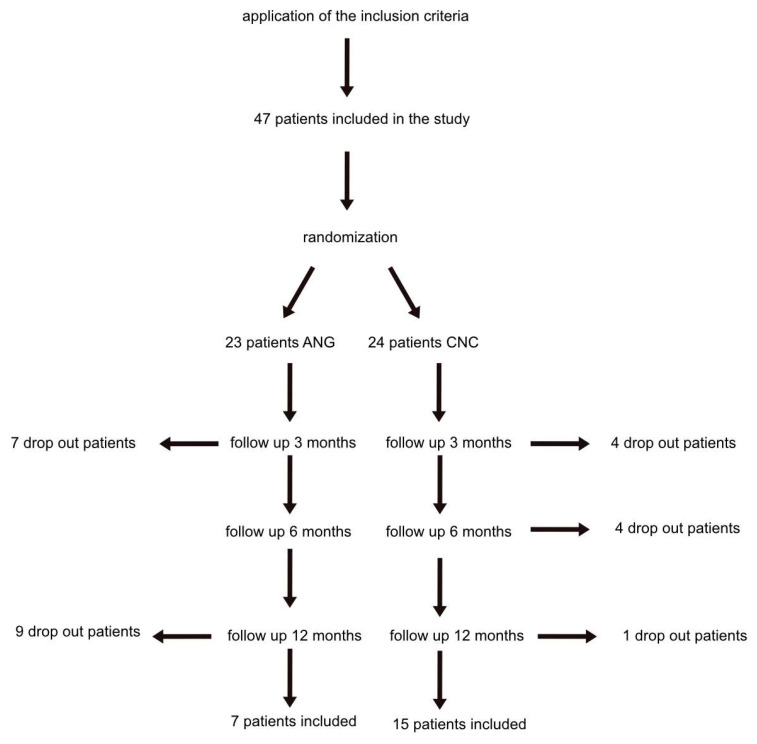
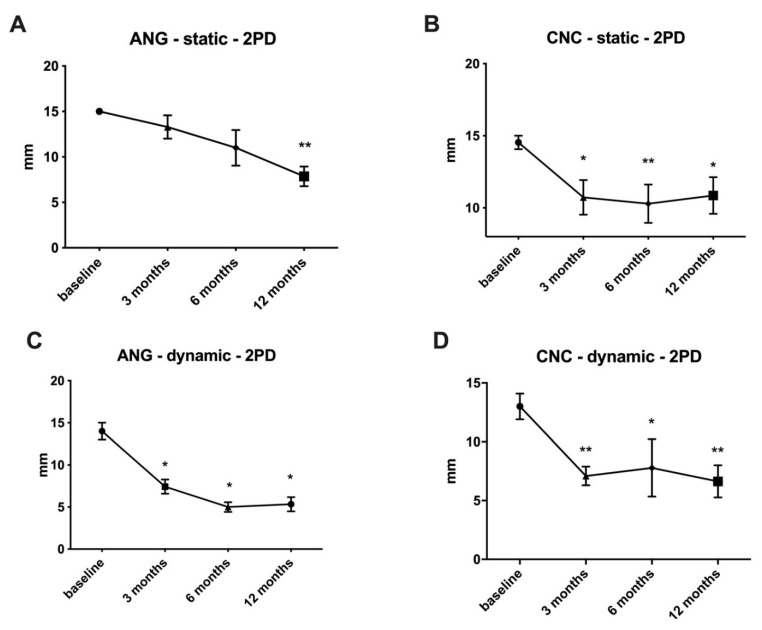
Introduction: If tensionless nerve coaptation is not possible, bridging the resulting peripheral nerve defect with an autologous nerve graft is still the current gold standard. The concept of conduits as an alternative with different materials and architectures, such as autologous vein conduits or bioartificial nerve conduits, could not replace the nerve graft until today. Chitosan, as a relatively new biomaterial, has recently demonstrated exceptional biocompatibility and material stability with neural lineage cells. The purpose of this prospective randomized clinical experiment was to determine the efficacy of chitosan-based nerve conduits in regenerating sensory nerves in the hand. Materials and methods: Forty-seven patients with peripheral nerve defects up to 26 mm distal to the carpal tunnel were randomized to receive either a chitosan conduit or an autologous nerve graft with the latter serving as the control group. Fifteen patients from the conduit group and seven patients from the control group were available for a 12-month follow-up examination. The primary outcome parameter was tactile gnosis measured with two-point discrimination. The secondary outcome parameters were Semmens Weinstein Monofilament Testing, self-assessed pain, and patient satisfaction. Results: Significant improvement (in static two-point discrimination) was observed six months after trauma (10.7 ± 1.2 mm; p < 0.05) for chitosan-based nerve conduits, but no further improvement was observed after 12 months of regeneration (10.9 ± 1.3 mm). After six months and twelve months, the autologous nerve graft demonstrated comparable results to the nerve conduit, with a static two-point discrimination of 11.0 ± 2.0 mm and 7.9 ± 1.1 mm. Semmes Weinstein Filament Testing in the nerve conduit group showed a continuous improvement over the regeneration period by reaching from 3.1 ± 0.3 after three months up to 3.7 ± 0.4 after twelve months. Autologous nerve grafts presented similar results: 3.3 ± 0.4 after three months and 3.7 ± 0.5 after twelve months. Patient satisfaction and self-reported pain levels were similar between the chitosan nerve conduit and nerve graft groups. One patient required revision surgery due to complications associated with the chitosan nerve tube. Conclusion: Chitosan-based nerve conduits are safe and suitable for bridging nerve lesions up to 26 mm in the hand. Tactile gnosis improved significantly during the early regeneration period, and functional outcomes were similar to those obtained with an autologous nerve graft. Thus, chitosan appears to be a sufficient substitute for autologous nerve grafts in the treatment of small nerve defects in the hand.
如果无法进行无张力神经吻合,用自体神经移植物桥接由此产生的周围神经缺损仍是当前的金标准。直到如今,使用不同材料和结构的导管(如自体静脉导管或生物人工神经导管)作为替代物的概念仍无法取代神经移植物。壳聚糖作为一种相对较新的生物材料,最近已证明与神经谱系细胞具有卓越的生物相容性和材料稳定性。这项前瞻性随机临床试验的目的是确定基于壳聚糖的神经导管对手部感觉神经再生的疗效。
47例腕管远侧26毫米以内周围神经缺损的患者被随机分组,分别接受壳聚糖导管或自体神经移植物,后者作为对照组。导管组有15例患者和对照组有7例患者可进行为期12个月的随访检查。主要结局参数是用两点辨别法测量的触觉识别。次要结局参数是Semmens Weinstein单丝测试、自我评估的疼痛和患者满意度。
基于壳聚糖的神经导管在创伤后6个月时(静态两点辨别法)有显著改善(10.7±1.2毫米;p<0.05),但再生12个月后未观察到进一步改善(10.9±1.3毫米)。6个月和12个月后,自体神经移植物与神经导管的结果相当,静态两点辨别法分别为11.0±2.0毫米和7.9±1.1毫米。神经导管组的Semmes Weinstein单丝测试显示在整个再生期持续改善,从3个月时的3.1±0.3提高到12个月时的3.7±0.4。自体神经移植物呈现类似结果:3个月时为3.3±0.4,12个月时为3.7±0.5。壳聚糖神经导管组和神经移植物组的患者满意度和自我报告的疼痛程度相似。1例患者因与壳聚糖神经管相关的并发症需要进行翻修手术。
基于壳聚糖的神经导管安全且适用于桥接手部长达26毫米的神经损伤。在早期再生期触觉识别有显著改善,功能结局与自体神经移植物相似。因此,在治疗手部小神经缺损时,壳聚糖似乎是自体神经移植物的充分替代品。